 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeNicolas Padoy
Weakly Supervised Temporal Convolutional Networks for Fine-grained Surgical Activity Recognition
Feb 21, 2023
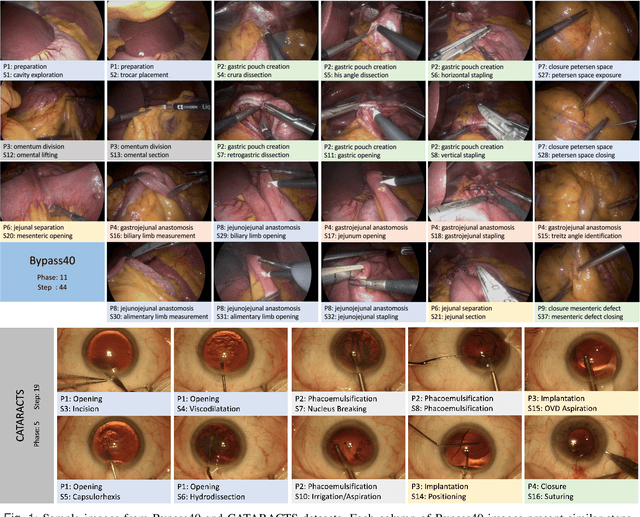
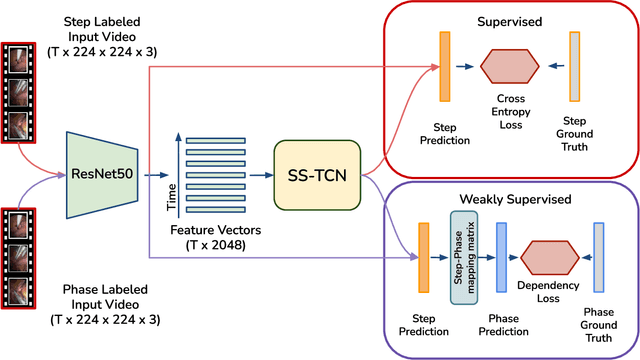
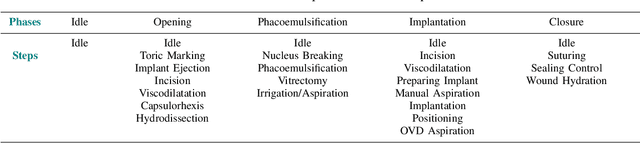
Automatic recognition of fine-grained surgical activities, called steps, is a challenging but crucial task for intelligent intra-operative computer assistance. The development of current vision-based activity recognition methods relies heavily on a high volume of manually annotated data. This data is difficult and time-consuming to generate and requires domain-specific knowledge. In this work, we propose to use coarser and easier-to-annotate activity labels, namely phases, as weak supervision to learn step recognition with fewer step annotated videos. We introduce a step-phase dependency loss to exploit the weak supervision signal. We then employ a Single-Stage Temporal Convolutional Network (SS-TCN) with a ResNet-50 backbone, trained in an end-to-end fashion from weakly annotated videos, for temporal activity segmentation and recognition. We extensively evaluate and show the effectiveness of the proposed method on a large video dataset consisting of 40 laparoscopic gastric bypass procedures and the public benchmark CATARACTS containing 50 cataract surgeries.
CholecTriplet2022: Show me a tool and tell me the triplet -- an endoscopic vision challenge for surgical action triplet detection
Feb 13, 2023
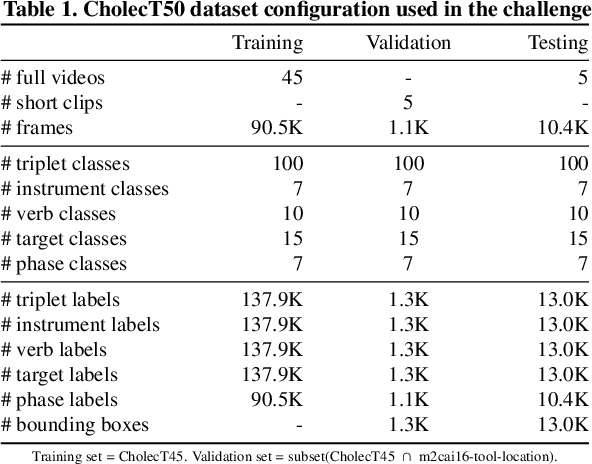
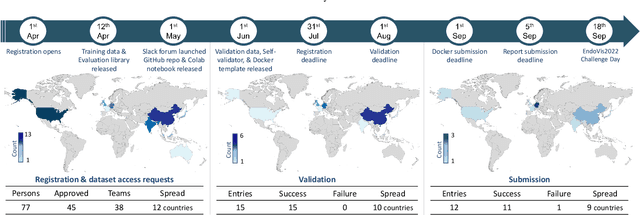
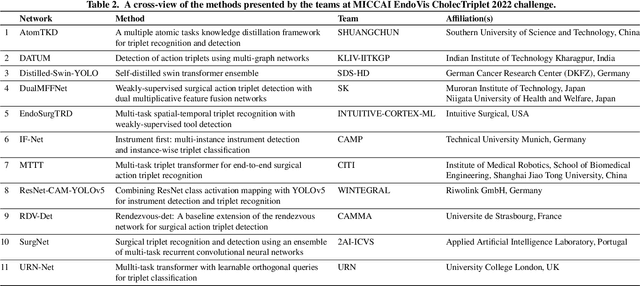
Formalizing surgical activities as triplets of the used instruments, actions performed, and target anatomies is becoming a gold standard approach for surgical activity modeling. The benefit is that this formalization helps to obtain a more detailed understanding of tool-tissue interaction which can be used to develop better Artificial Intelligence assistance for image-guided surgery. Earlier efforts and the CholecTriplet challenge introduced in 2021 have put together techniques aimed at recognizing these triplets from surgical footage. Estimating also the spatial locations of the triplets would offer a more precise intraoperative context-aware decision support for computer-assisted intervention. This paper presents the CholecTriplet2022 challenge, which extends surgical action triplet modeling from recognition to detection. It includes weakly-supervised bounding box localization of every visible surgical instrument (or tool), as the key actors, and the modeling of each tool-activity in the form of <instrument, verb, target> triplet. The paper describes a baseline method and 10 new deep learning algorithms presented at the challenge to solve the task. It also provides thorough methodological comparisons of the methods, an in-depth analysis of the obtained results, their significance, and useful insights for future research directions and applications in surgery.
Preserving Privacy in Surgical Video Analysis Using Artificial Intelligence: A Deep Learning Classifier to Identify Out-of-Body Scenes in Endoscopic Videos
Jan 17, 2023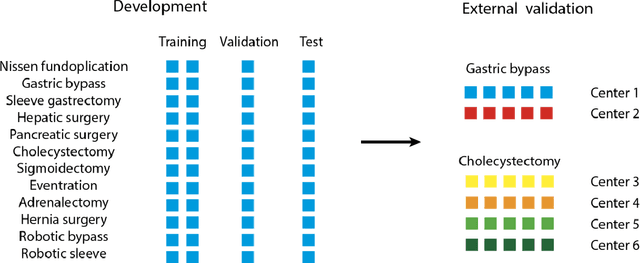
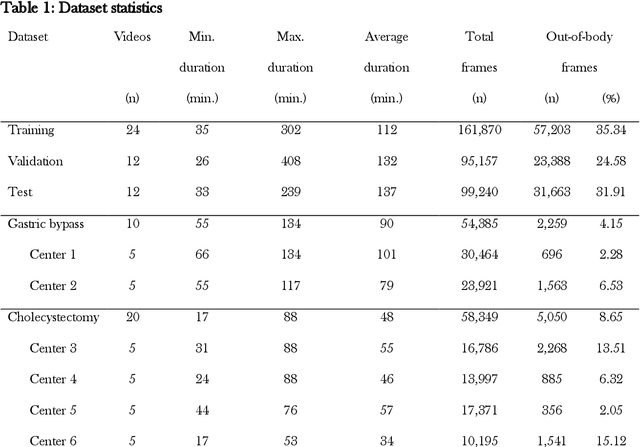
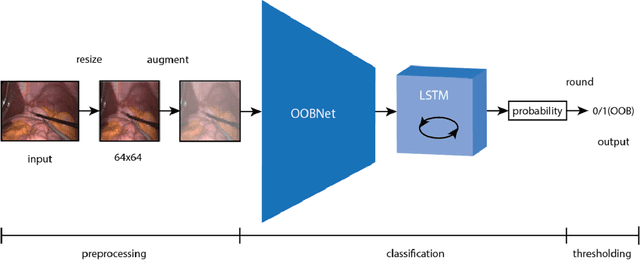
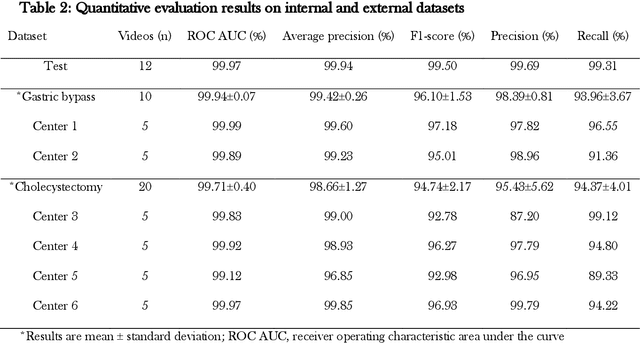
Objective: To develop and validate a deep learning model for the identification of out-of-body images in endoscopic videos. Background: Surgical video analysis facilitates education and research. However, video recordings of endoscopic surgeries can contain privacy-sensitive information, especially if out-of-body scenes are recorded. Therefore, identification of out-of-body scenes in endoscopic videos is of major importance to preserve the privacy of patients and operating room staff. Methods: A deep learning model was trained and evaluated on an internal dataset of 12 different types of laparoscopic and robotic surgeries. External validation was performed on two independent multicentric test datasets of laparoscopic gastric bypass and cholecystectomy surgeries. All images extracted from the video datasets were annotated as inside or out-of-body. Model performance was evaluated compared to human ground truth annotations measuring the receiver operating characteristic area under the curve (ROC AUC). Results: The internal dataset consisting of 356,267 images from 48 videos and the two multicentric test datasets consisting of 54,385 and 58,349 images from 10 and 20 videos, respectively, were annotated. Compared to ground truth annotations, the model identified out-of-body images with 99.97% ROC AUC on the internal test dataset. Mean $\pm$ standard deviation ROC AUC on the multicentric gastric bypass dataset was 99.94$\pm$0.07% and 99.71$\pm$0.40% on the multicentric cholecystectomy dataset, respectively. Conclusion: The proposed deep learning model can reliably identify out-of-body images in endoscopic videos. The trained model is publicly shared. This facilitates privacy preservation in surgical video analysis.
Biomedical image analysis competitions: The state of current participation practice
Dec 16, 2022The number of international benchmarking competitions is steadily increasing in various fields of machine learning (ML) research and practice. So far, however, little is known about the common practice as well as bottlenecks faced by the community in tackling the research questions posed. To shed light on the status quo of algorithm development in the specific field of biomedical imaging analysis, we designed an international survey that was issued to all participants of challenges conducted in conjunction with the IEEE ISBI 2021 and MICCAI 2021 conferences (80 competitions in total). The survey covered participants' expertise and working environments, their chosen strategies, as well as algorithm characteristics. A median of 72% challenge participants took part in the survey. According to our results, knowledge exchange was the primary incentive (70%) for participation, while the reception of prize money played only a minor role (16%). While a median of 80 working hours was spent on method development, a large portion of participants stated that they did not have enough time for method development (32%). 25% perceived the infrastructure to be a bottleneck. Overall, 94% of all solutions were deep learning-based. Of these, 84% were based on standard architectures. 43% of the respondents reported that the data samples (e.g., images) were too large to be processed at once. This was most commonly addressed by patch-based training (69%), downsampling (37%), and solving 3D analysis tasks as a series of 2D tasks. K-fold cross-validation on the training set was performed by only 37% of the participants and only 50% of the participants performed ensembling based on multiple identical models (61%) or heterogeneous models (39%). 48% of the respondents applied postprocessing steps.
Real-Time Artificial Intelligence Assistance for Safe Laparoscopic Cholecystectomy: Early-Stage Clinical Evaluation
Dec 13, 2022
Artificial intelligence is set to be deployed in operating rooms to improve surgical care. This early-stage clinical evaluation shows the feasibility of concurrently attaining real-time, high-quality predictions from several deep neural networks for endoscopic video analysis deployed for assistance during three laparoscopic cholecystectomies.
Latent Graph Representations for Critical View of Safety Assessment
Dec 08, 2022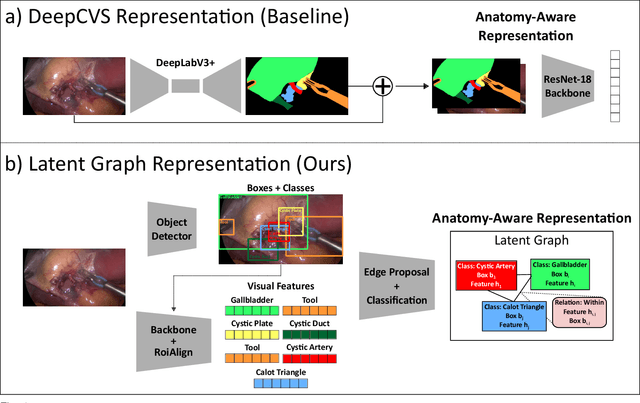
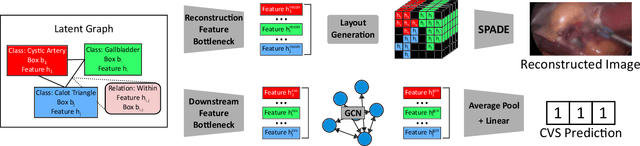
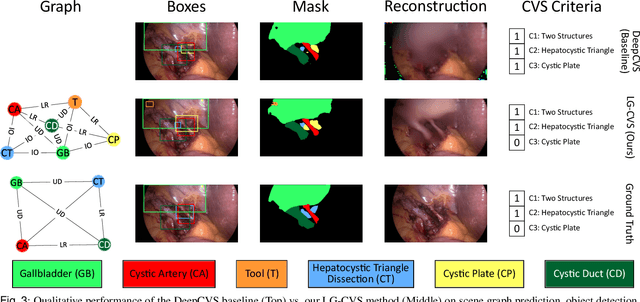
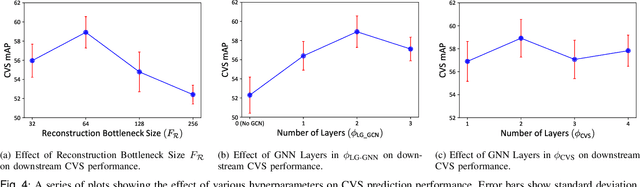
Assessing the critical view of safety in laparoscopic cholecystectomy requires accurate identification and localization of key anatomical structures, reasoning about their geometric relationships to one another, and determining the quality of their exposure. In this work, we propose to capture each of these aspects by modeling the surgical scene with a disentangled latent scene graph representation, which we can then process using a graph neural network. Unlike previous approaches using graph representations, we explicitly encode in our graphs semantic information such as object locations and shapes, class probabilities and visual features. We also incorporate an auxiliary image reconstruction objective to help train the latent graph representations. We demonstrate the value of these components through comprehensive ablation studies and achieve state-of-the-art results for critical view of safety prediction across multiple experimental settings.
Rendezvous in Time: An Attention-based Temporal Fusion approach for Surgical Triplet Recognition
Nov 30, 2022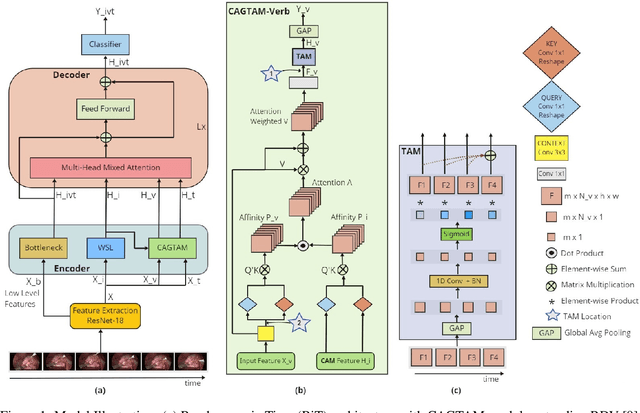

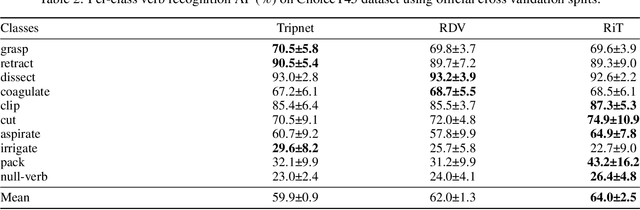
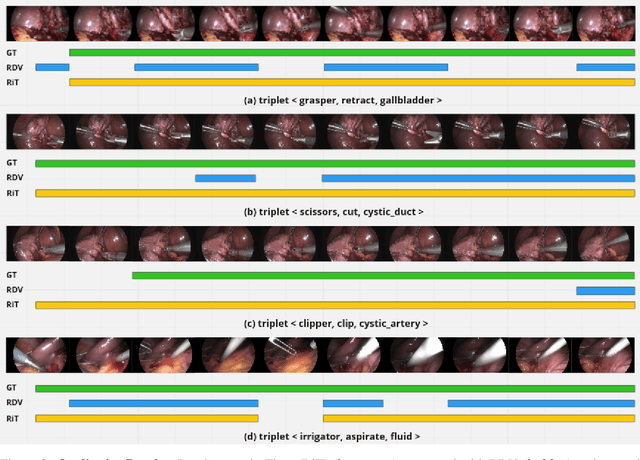
One of the recent advances in surgical AI is the recognition of surgical activities as triplets of (instrument, verb, target). Albeit providing detailed information for computer-assisted intervention, current triplet recognition approaches rely only on single frame features. Exploiting the temporal cues from earlier frames would improve the recognition of surgical action triplets from videos. In this paper, we propose Rendezvous in Time (RiT) - a deep learning model that extends the state-of-the-art model, Rendezvous, with temporal modeling. Focusing more on the verbs, our RiT explores the connectedness of current and past frames to learn temporal attention-based features for enhanced triplet recognition. We validate our proposal on the challenging surgical triplet dataset, CholecT45, demonstrating an improved recognition of the verb and triplet along with other interactions involving the verb such as (instrument, verb). Qualitative results show that the RiT produces smoother predictions for most triplet instances than the state-of-the-arts. We present a novel attention-based approach that leverages the temporal fusion of video frames to model the evolution of surgical actions and exploit their benefits for surgical triplet recognition.
Dissecting Self-Supervised Learning Methods for Surgical Computer Vision
Jul 01, 2022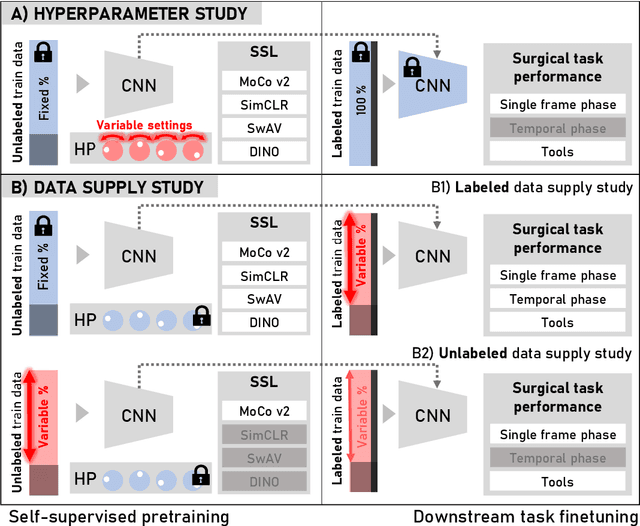
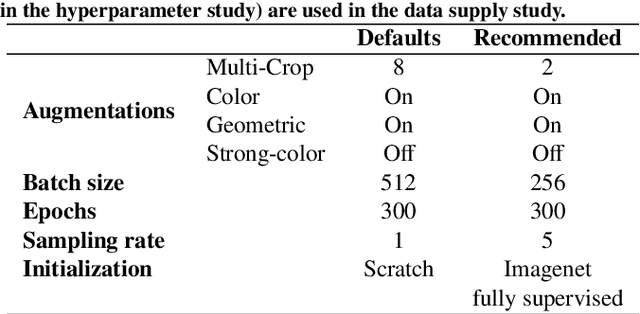
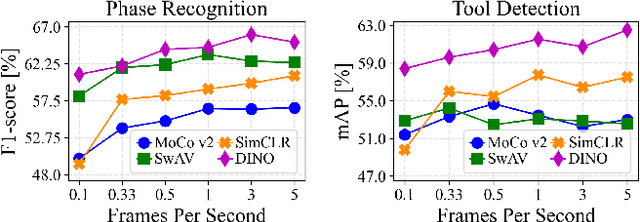
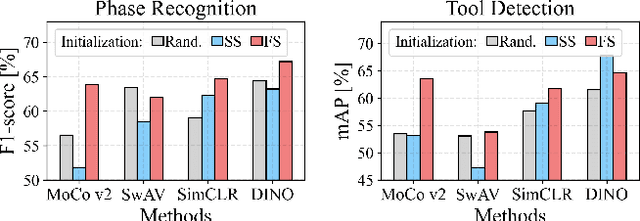
The field of surgical computer vision has undergone considerable breakthroughs in recent years with the rising popularity of deep neural network-based methods. However, standard fully-supervised approaches for training such models require vast amounts of annotated data, imposing a prohibitively high cost; especially in the clinical domain. Self-Supervised Learning (SSL) methods, which have begun to gain traction in the general computer vision community, represent a potential solution to these annotation costs, allowing to learn useful representations from only unlabeled data. Still, the effectiveness of SSL methods in more complex and impactful domains, such as medicine and surgery, remains limited and unexplored. In this work, we address this critical need by investigating four state-of-the-art SSL methods (MoCo v2, SimCLR, DINO, SwAV) in the context of surgical computer vision. We present an extensive analysis of the performance of these methods on the Cholec80 dataset for two fundamental and popular tasks in surgical context understanding, phase recognition and tool presence detection. We examine their parameterization, then their behavior with respect to training data quantities in semi-supervised settings. Correct transfer of these methods to surgery, as described and conducted in this work, leads to substantial performance gains over generic uses of SSL - up to 7% on phase recognition and 20% on tool presence detection - as well as state-of-the-art semi-supervised phase recognition approaches by up to 14%. The code will be made available at https://github.com/CAMMA-public/SelfSupSurg.
Data Splits and Metrics for Method Benchmarking on Surgical Action Triplet Datasets
Apr 11, 2022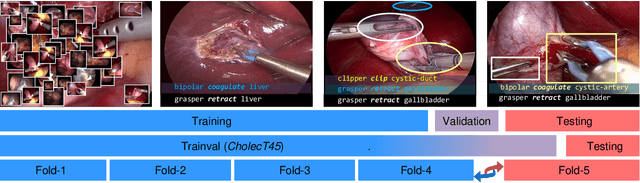


In addition to generating data and annotations, devising sensible data splitting strategies and evaluation metrics is essential for the creation of a benchmark dataset. This practice ensures consensus on the usage of the data, homogeneous assessment, and uniform comparison of research methods on the dataset. This study focuses on CholecT50, which is a 50 video surgical dataset that formalizes surgical activities as triplets of <instrument, verb, target>. In this paper, we introduce the standard splits for the CholecT50 and CholecT45 datasets and show how they compare with existing use of the dataset. CholecT45 is the first public release of 45 videos of CholecT50 dataset. We also develop a metrics library, ivtmetrics, for model evaluation on surgical triplets. Furthermore, we conduct a benchmark study by reproducing baseline methods in the most predominantly used deep learning frameworks (PyTorch and TensorFlow) to evaluate them using the proposed data splits and metrics and release them publicly to support future research. The proposed data splits and evaluation metrics will enable global tracking of research progress on the dataset and facilitate optimal model selection for further deployment.
CholecTriplet2021: A benchmark challenge for surgical action triplet recognition
Apr 10, 2022

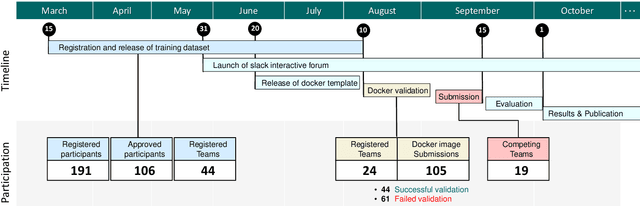
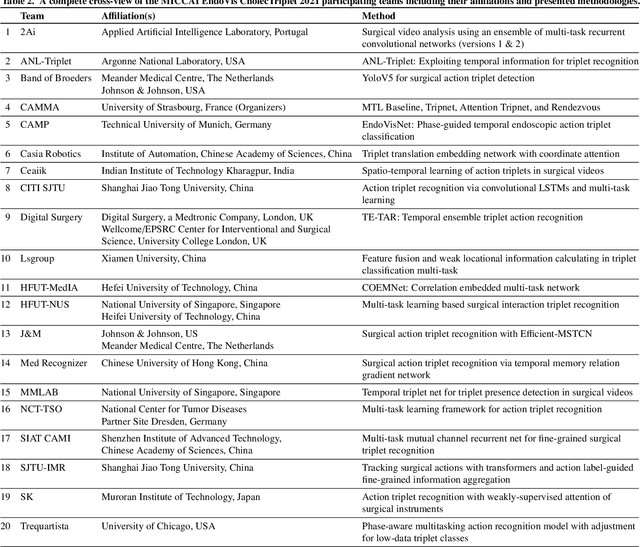
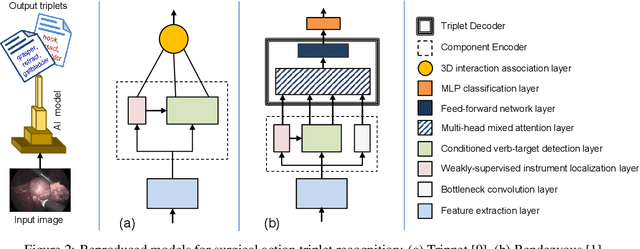
Context-aware decision support in the operating room can foster surgical safety and efficiency by leveraging real-time feedback from surgical workflow analysis. Most existing works recognize surgical activities at a coarse-grained level, such as phases, steps or events, leaving out fine-grained interaction details about the surgical activity; yet those are needed for more helpful AI assistance in the operating room. Recognizing surgical actions as triplets of <instrument, verb, target> combination delivers comprehensive details about the activities taking place in surgical videos. This paper presents CholecTriplet2021: an endoscopic vision challenge organized at MICCAI 2021 for the recognition of surgical action triplets in laparoscopic videos. The challenge granted private access to the large-scale CholecT50 dataset, which is annotated with action triplet information. In this paper, we present the challenge setup and assessment of the state-of-the-art deep learning methods proposed by the participants during the challenge. A total of 4 baseline methods from the challenge organizers and 19 new deep learning algorithms by competing teams are presented to recognize surgical action triplets directly from surgical videos, achieving mean average precision (mAP) ranging from 4.2% to 38.1%. This study also analyzes the significance of the results obtained by the presented approaches, performs a thorough methodological comparison between them, in-depth result analysis, and proposes a novel ensemble method for enhanced recognition. Our analysis shows that surgical workflow analysis is not yet solved, and also highlights interesting directions for future research on fine-grained surgical activity recognition which is of utmost importance for the development of AI in surgery.