 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeBenchX: Benchmarking AI Models for Cancer Detection and Localization with Demographic and Protocol Biases
Jun 23, 2026Artificial intelligence (AI) has achieved remarkable success in medical imaging, but it is widely recognized that these models often perform inconsistently across real-world clinical settings. Such inconsistencies occur when patient demographics and imaging protocols vary, for example, in detecting small tumors, analyzing scans from different contrast phases, or evaluating patients of different ages or sexes. To quantify these inconsistencies, we develop a large-scale, open benchmark of 85,355 CT scans that systematically evaluates 12 tumor-detection AI models across tumor size, location, patient subgroup, and imaging protocol. We leverage large language models (LLMs) to extract and organize subgroup information from clinical data, which makes the analysis both scalable and reproducible. Our benchmark reveals that current state-of-the-art AI models, optimized for average accuracy, perform poorly in rare or underrepresented subgroups, such as young, female African Americans. However, collecting sufficient annotated data for these rare cases is often impractical. The benchmark provides a foundation for building more reliable and robust AI models for tumor detection and highlighting the need for rigorous, subgroup-level evaluation in medical imaging and computer vision. Datasets, code
RadThinking: A Dataset for Longitudinal Clinical Reasoning in Radiology
May 11, 2026Cancer screening is a reasoning task. A radiologist observes findings, compares them to prior scans, integrates clinical context, and reaches a diagnostic conclusion confirmed by pathology. We present RadThinking, a Visual Question Answering (VQA) dataset that makes this reasoning explicit and trainable. RadThinking releases VQA pairs at three difficulty tiers. Foundation VQAs are atomic perception questions. Single-step reasoning VQAs apply one clinical rule. Compositional VQAs require multi-step chain-of-thought to reach a guideline category such as LI-RADS-5. For every compositional VQA, we release the chain of foundation VQAs that solves it. The chain follows the rules of the governing clinical reporting standard. The dataset spans 20,362 CT scans from 9,131 patients across 43 cancer groups, plus 2,077 verified healthy controls with >1-year follow-up. To our knowledge, RadThinking is the first cancer-screening VQA corpus that stratifies questions by reasoning depth and grounds compositions in clinical reporting standards. The foundation tier supplies atomic perception supervision. The compositional tier supplies chain-of-thought data and verifiable rewards for reinforcement-learning recipes such as DeepSeek-R1 and OpenAI o1. RadThinking enables systematic training and evaluation of whether AI systems can reason about cancer, not merely detect it.
DeepTumorVQA: A Hierarchical 3D CT Benchmark for Stage-Wise Evaluation of Medical VLMs and Tool-Augmented Agents
May 10, 2026Medical vision-language models (VLMs) and AI agents have made significant progress in learning to analyze and reason about clinical images. However, existing medical visual question answering (VQA) benchmarks collapse model capabilities into a single accuracy score, obscuring where and why models fail. We propose DeepTumorVQA, a hierarchical benchmark that follows the multi-stage evidence chain in tumor diagnosis and decomposes 3D CT reasoning into four stages: recognition, measurement, visual reasoning, and medical reasoning. Higher-level questions remain independently scorable, while their ground-truth evidence chains are defined over lower-level primitives. The benchmark contains 476K questions across 42 clinical subtypes on 9,262 3D CT volumes. In addition to a direct reasoning mode for VLMs, DeepTumorVQA provides tool-interaction environments for agent evaluation, where a model can call external tools, including segmentation models, measurement programs, and medical knowledge modules, before answering the question. Evaluating over 30 model configurations, we find that reliable quantitative measurement is the primary bottleneck, making later-stage visual and medical reasoning harder for VLMs, while tool augmentation substantially mitigates this issue. When tools are available, leveraging medical knowledge and tools to reason about medical images becomes a new challenge. We further show that ground-truth step-by-step tool-use traces from DeepTumorVQA can supervise agents and reduce tool-use and reasoning failures. This stage-wise progression from recognition to measurement to visual and medical reasoning provides a concrete roadmap for future medical VLM and AI agent studies. All data and code are released at https://github.com/Schuture/DeepTumorVQA.
Distilling Photon-Counting CT into Routine Chest CT through Clinically Validated Degradation Modeling
Apr 08, 2026Photon-counting CT (PCCT) provides superior image quality with higher spatial resolution and lower noise compared to conventional energy-integrating CT (EICT), but its limited clinical availability restricts large-scale research and clinical deployment. To bridge this gap, we propose SUMI, a simulated degradation-to-enhancement method that learns to reverse realistic acquisition artifacts in low-quality EICT by leveraging high-quality PCCT as reference. Our central insight is to explicitly model realistic acquisition degradations, transforming PCCT into clinically plausible lower-quality counterparts and learning to invert this process. The simulated degradations were validated for clinical realism by board-certified radiologists, enabling faithful supervision without requiring paired acquisitions at scale. As outcomes of this technical contribution, we: (1) train a latent diffusion model on 1,046 PCCTs, using an autoencoder first pre-trained on both these PCCTs and 405,379 EICTs from 145 hospitals to extract general CT latent features that we release for reuse in other generative medical imaging tasks; (2) construct a large-scale dataset of over 17,316 publicly available EICTs enhanced to PCCT-like quality, with radiologist-validated voxel-wise annotations of airway trees, arteries, veins, lungs, and lobes; and (3) demonstrate substantial improvements: across external data, SUMI outperforms state-of-the-art image translation methods by 15% in SSIM and 20% in PSNR, improves radiologist-rated clinical utility in reader studies, and enhances downstream top-ranking lesion detection performance, increasing sensitivity by up to 15% and F1 score by up to 10%. Our results suggest that emerging imaging advances can be systematically distilled into routine EICT using limited high-quality scans as reference.
Early and Prediagnostic Detection of Pancreatic Cancer from Computed Tomography
Jan 29, 2026Pancreatic ductal adenocarcinoma (PDAC), one of the deadliest solid malignancies, is often detected at a late and inoperable stage. Retrospective reviews of prediagnostic CT scans, when conducted by expert radiologists aware that the patient later developed PDAC, frequently reveal lesions that were previously overlooked. To help detecting these lesions earlier, we developed an automated system named ePAI (early Pancreatic cancer detection with Artificial Intelligence). It was trained on data from 1,598 patients from a single medical center. In the internal test involving 1,009 patients, ePAI achieved an area under the receiver operating characteristic curve (AUC) of 0.939-0.999, a sensitivity of 95.3%, and a specificity of 98.7% for detecting small PDAC less than 2 cm in diameter, precisely localizing PDAC as small as 2 mm. In an external test involving 7,158 patients across 6 centers, ePAI achieved an AUC of 0.918-0.945, a sensitivity of 91.5%, and a specificity of 88.0%, precisely localizing PDAC as small as 5 mm. Importantly, ePAI detected PDACs on prediagnostic CT scans obtained 3 to 36 months before clinical diagnosis that had originally been overlooked by radiologists. It successfully detected and localized PDACs in 75 of 159 patients, with a median lead time of 347 days before clinical diagnosis. Our multi-reader study showed that ePAI significantly outperformed 30 board-certified radiologists by 50.3% (P < 0.05) in sensitivity while maintaining a comparable specificity of 95.4% in detecting PDACs early and prediagnostic. These findings suggest its potential of ePAI as an assistive tool to improve early detection of pancreatic cancer.
See More, Change Less: Anatomy-Aware Diffusion for Contrast Enhancement
Dec 08, 2025Image enhancement improves visual quality and helps reveal details that are hard to see in the original image. In medical imaging, it can support clinical decision-making, but current models often over-edit. This can distort organs, create false findings, and miss small tumors because these models do not understand anatomy or contrast dynamics. We propose SMILE, an anatomy-aware diffusion model that learns how organs are shaped and how they take up contrast. It enhances only clinically relevant regions while leaving all other areas unchanged. SMILE introduces three key ideas: (1) structure-aware supervision that follows true organ boundaries and contrast patterns; (2) registration-free learning that works directly with unaligned multi-phase CT scans; (3) unified inference that provides fast and consistent enhancement across all contrast phases. Across six external datasets, SMILE outperforms existing methods in image quality (14.2% higher SSIM, 20.6% higher PSNR, 50% better FID) and in clinical usefulness by producing anatomically accurate and diagnostically meaningful images. SMILE also improves cancer detection from non-contrast CT, raising the F1 score by up to 10 percent.
PanTS: The Pancreatic Tumor Segmentation Dataset
Jul 02, 2025PanTS is a large-scale, multi-institutional dataset curated to advance research in pancreatic CT analysis. It contains 36,390 CT scans from 145 medical centers, with expert-validated, voxel-wise annotations of over 993,000 anatomical structures, covering pancreatic tumors, pancreas head, body, and tail, and 24 surrounding anatomical structures such as vascular/skeletal structures and abdominal/thoracic organs. Each scan includes metadata such as patient age, sex, diagnosis, contrast phase, in-plane spacing, slice thickness, etc. AI models trained on PanTS achieve significantly better performance in pancreatic tumor detection, localization, and segmentation compared to those trained on existing public datasets. Our analysis indicates that these gains are directly attributable to the 16x larger-scale tumor annotations and indirectly supported by the 24 additional surrounding anatomical structures. As the largest and most comprehensive resource of its kind, PanTS offers a new benchmark for developing and evaluating AI models in pancreatic CT analysis.
Are Vision Language Models Ready for Clinical Diagnosis? A 3D Medical Benchmark for Tumor-centric Visual Question Answering
May 25, 2025Vision-Language Models (VLMs) have shown promise in various 2D visual tasks, yet their readiness for 3D clinical diagnosis remains unclear due to stringent demands for recognition precision, reasoning ability, and domain knowledge. To systematically evaluate these dimensions, we present DeepTumorVQA, a diagnostic visual question answering (VQA) benchmark targeting abdominal tumors in CT scans. It comprises 9,262 CT volumes (3.7M slices) from 17 public datasets, with 395K expert-level questions spanning four categories: Recognition, Measurement, Visual Reasoning, and Medical Reasoning. DeepTumorVQA introduces unique challenges, including small tumor detection and clinical reasoning across 3D anatomy. Benchmarking four advanced VLMs (RadFM, M3D, Merlin, CT-CHAT), we find current models perform adequately on measurement tasks but struggle with lesion recognition and reasoning, and are still not meeting clinical needs. Two key insights emerge: (1) large-scale multimodal pretraining plays a crucial role in DeepTumorVQA testing performance, making RadFM stand out among all VLMs. (2) Our dataset exposes critical differences in VLM components, where proper image preprocessing and design of vision modules significantly affect 3D perception. To facilitate medical multimodal research, we have released DeepTumorVQA as a rigorous benchmark: https://github.com/Schuture/DeepTumorVQA.
ScaleMAI: Accelerating the Development of Trusted Datasets and AI Models
Jan 06, 2025



Building trusted datasets is critical for transparent and responsible Medical AI (MAI) research, but creating even small, high-quality datasets can take years of effort from multidisciplinary teams. This process often delays AI benefits, as human-centric data creation and AI-centric model development are treated as separate, sequential steps. To overcome this, we propose ScaleMAI, an agent of AI-integrated data curation and annotation, allowing data quality and AI performance to improve in a self-reinforcing cycle and reducing development time from years to months. We adopt pancreatic tumor detection as an example. First, ScaleMAI progressively creates a dataset of 25,362 CT scans, including per-voxel annotations for benign/malignant tumors and 24 anatomical structures. Second, through progressive human-in-the-loop iterations, ScaleMAI provides Flagship AI Model that can approach the proficiency of expert annotators (30-year experience) in detecting pancreatic tumors. Flagship Model significantly outperforms models developed from smaller, fixed-quality datasets, with substantial gains in tumor detection (+14%), segmentation (+5%), and classification (72%) on three prestigious benchmarks. In summary, ScaleMAI transforms the speed, scale, and reliability of medical dataset creation, paving the way for a variety of impactful, data-driven applications.
Using AI for Mitigating the Impact of Network Delay in Cloud-based Intelligent Traffic Signal Control
Mar 06, 2020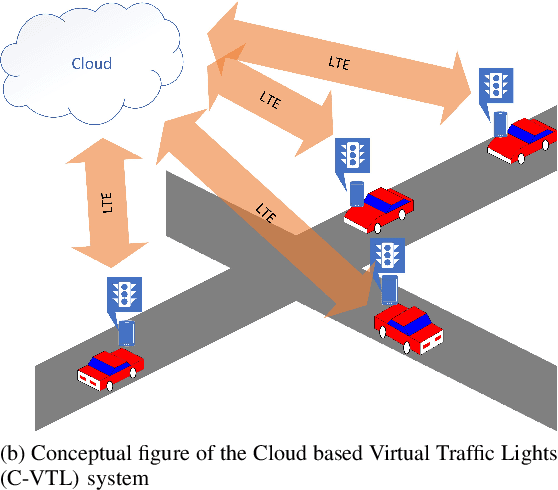
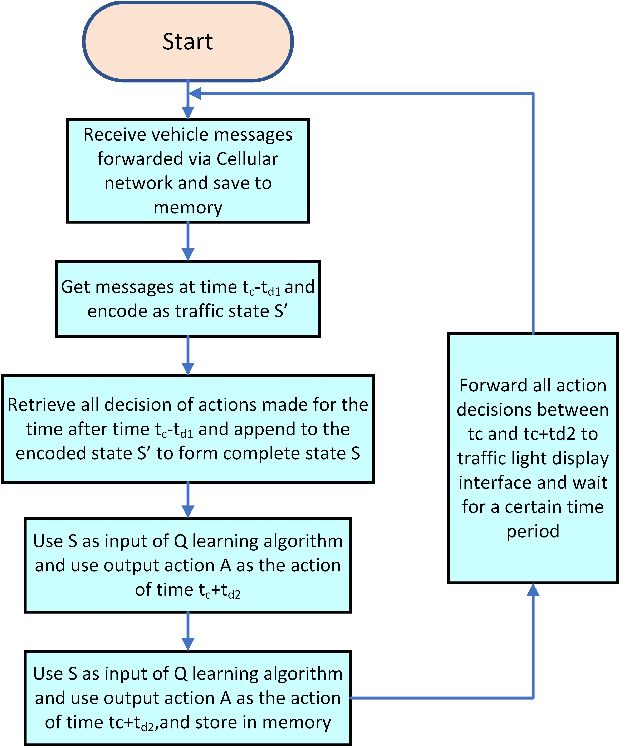
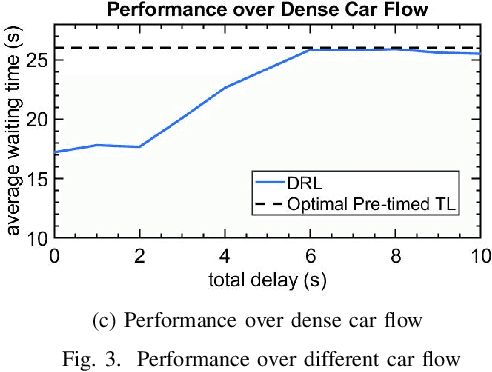
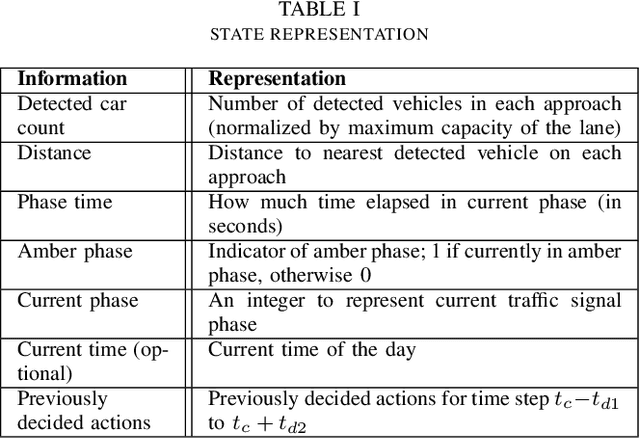
The recent advancements in cloud services, Internet of Things (IoT) and Cellular networks have made cloud computing an attractive option for intelligent traffic signal control (ITSC). Such a method significantly reduces the cost of cables, installation, number of devices used, and maintenance. ITSC systems based on cloud computing lower the cost of the ITSC systems and make it possible to scale the system by utilizing the existing powerful cloud platforms. While such systems have significant potential, one of the critical problems that should be addressed is the network delay. It is well known that network delay in message propagation is hard to prevent, which could potentially degrade the performance of the system or even create safety issues for vehicles at intersections. In this paper, we introduce a new traffic signal control algorithm based on reinforcement learning, which performs well even under severe network delay. The framework introduced in this paper can be helpful for all agent-based systems using remote computing resources where network delay could be a critical concern. Extensive simulation results obtained for different scenarios show the viability of the designed algorithm to cope with network delay.