 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeComparative Validation of Machine Learning Algorithms for Surgical Workflow and Skill Analysis with the HeiChole Benchmark
Sep 30, 2021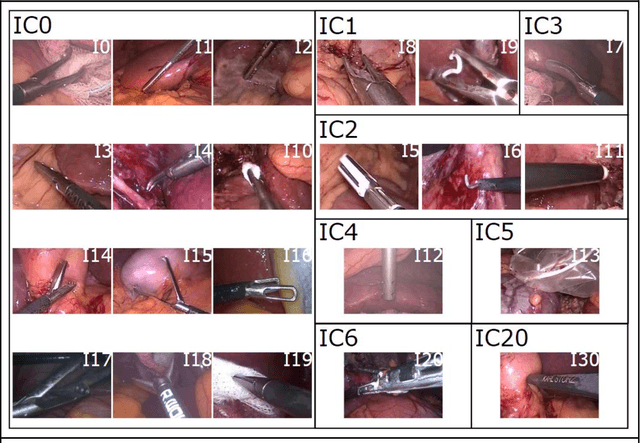
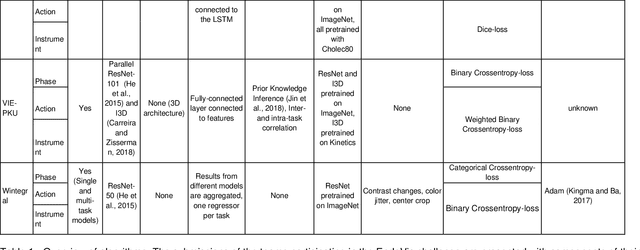
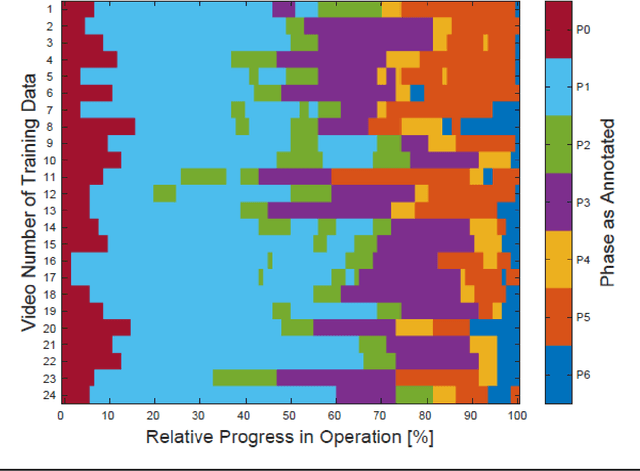
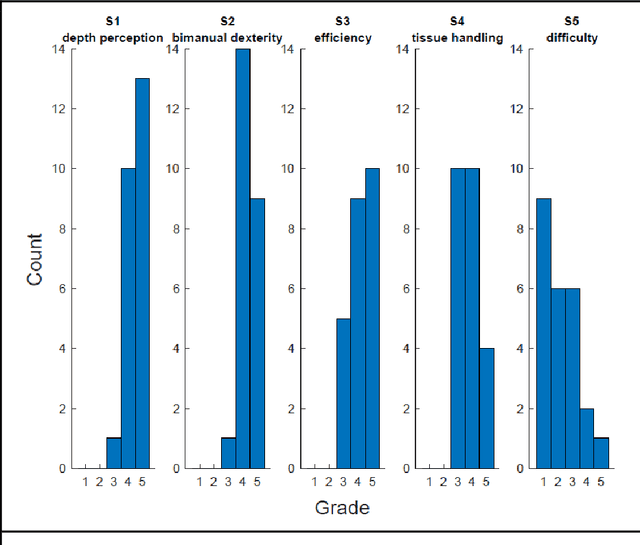
PURPOSE: Surgical workflow and skill analysis are key technologies for the next generation of cognitive surgical assistance systems. These systems could increase the safety of the operation through context-sensitive warnings and semi-autonomous robotic assistance or improve training of surgeons via data-driven feedback. In surgical workflow analysis up to 91% average precision has been reported for phase recognition on an open data single-center dataset. In this work we investigated the generalizability of phase recognition algorithms in a multi-center setting including more difficult recognition tasks such as surgical action and surgical skill. METHODS: To achieve this goal, a dataset with 33 laparoscopic cholecystectomy videos from three surgical centers with a total operation time of 22 hours was created. Labels included annotation of seven surgical phases with 250 phase transitions, 5514 occurences of four surgical actions, 6980 occurences of 21 surgical instruments from seven instrument categories and 495 skill classifications in five skill dimensions. The dataset was used in the 2019 Endoscopic Vision challenge, sub-challenge for surgical workflow and skill analysis. Here, 12 teams submitted their machine learning algorithms for recognition of phase, action, instrument and/or skill assessment. RESULTS: F1-scores were achieved for phase recognition between 23.9% and 67.7% (n=9 teams), for instrument presence detection between 38.5% and 63.8% (n=8 teams), but for action recognition only between 21.8% and 23.3% (n=5 teams). The average absolute error for skill assessment was 0.78 (n=1 team). CONCLUSION: Surgical workflow and skill analysis are promising technologies to support the surgical team, but are not solved yet, as shown by our comparison of algorithms. This novel benchmark can be used for comparable evaluation and validation of future work.
Surgical Data Science -- from Concepts to Clinical Translation
Oct 30, 2020
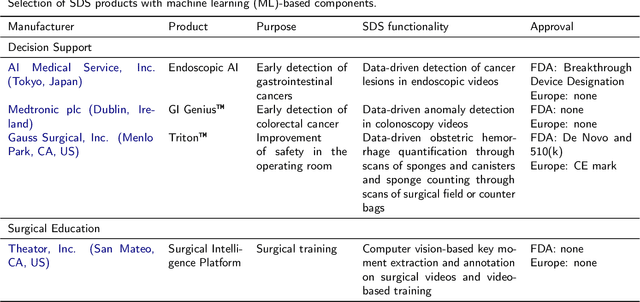
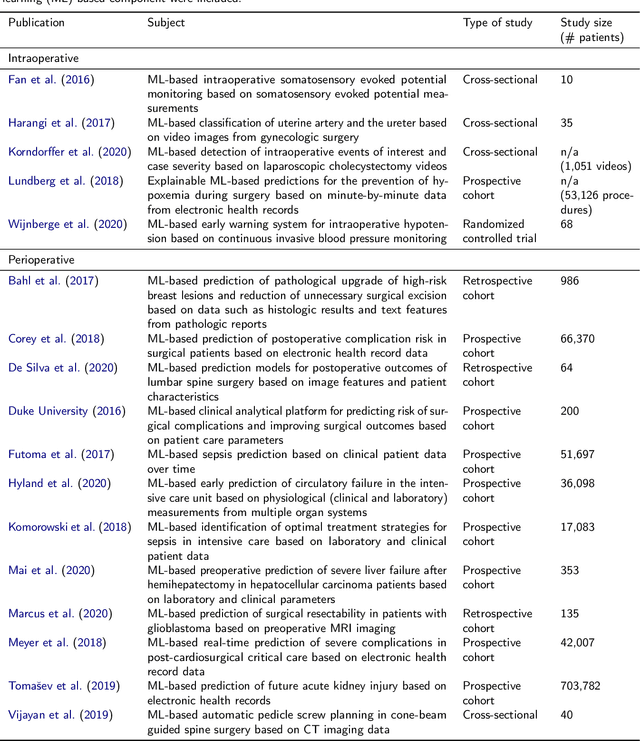
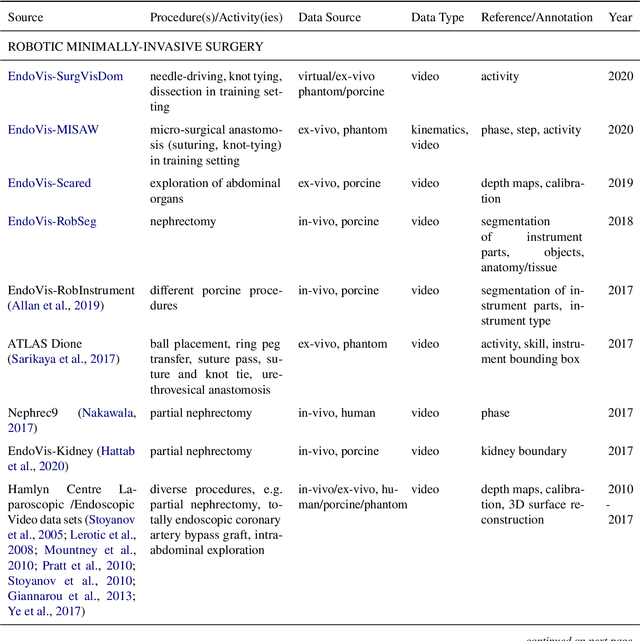
Recent developments in data science in general and machine learning in particular have transformed the way experts envision the future of surgery. Surgical data science is a new research field that aims to improve the quality of interventional healthcare through the capture, organization, analysis and modeling of data. While an increasing number of data-driven approaches and clinical applications have been studied in the fields of radiological and clinical data science, translational success stories are still lacking in surgery. In this publication, we shed light on the underlying reasons and provide a roadmap for future advances in the field. Based on an international workshop involving leading researchers in the field of surgical data science, we review current practice, key achievements and initiatives as well as available standards and tools for a number of topics relevant to the field, namely (1) technical infrastructure for data acquisition, storage and access in the presence of regulatory constraints, (2) data annotation and sharing and (3) data analytics. Drawing from this extensive review, we present current challenges for technology development and (4) describe a roadmap for faster clinical translation and exploitation of the full potential of surgical data science.
Heidelberg Colorectal Data Set for Surgical Data Science in the Sensor Operating Room
May 28, 2020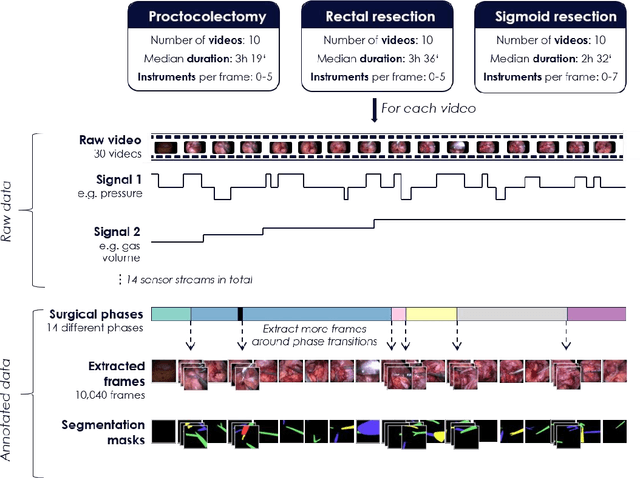
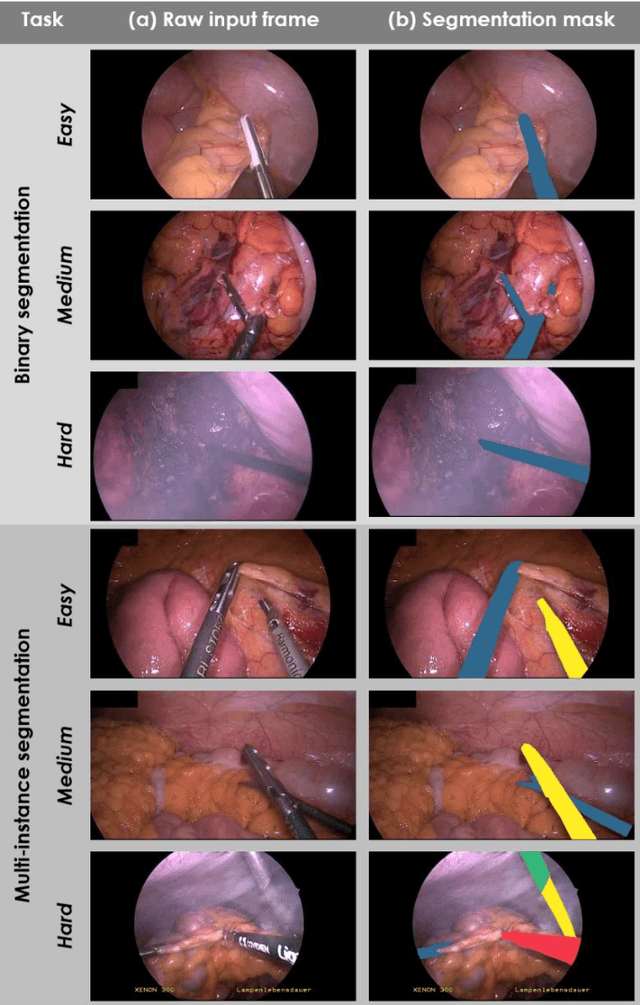
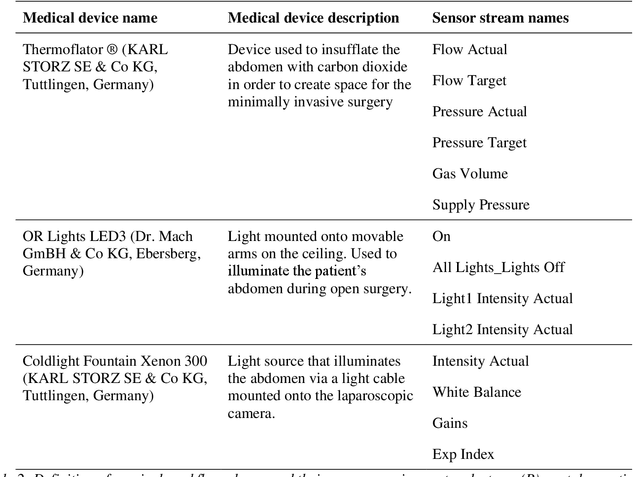
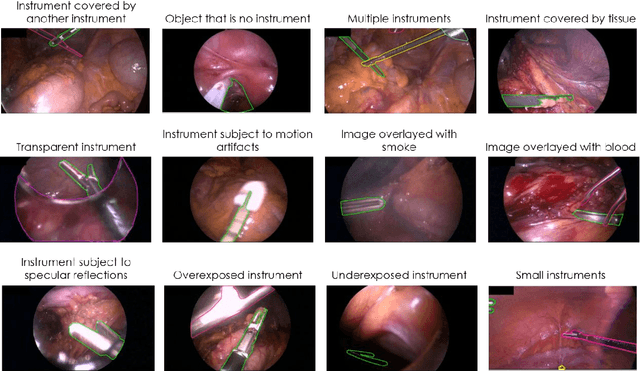
Image-based tracking of medical instruments is an integral part of many surgical data science applications. Previous research has addressed the tasks of detecting, segmenting and tracking medical instruments based on laparoscopic video data. However, the methods proposed still tend to fail when applied to challenging images and do not generalize well to data they have not been trained on. This paper introduces the Heidelberg Colorectal (HeiCo) data set - the first publicly available data set enabling comprehensive benchmarking of medical instrument detection and segmentation algorithms with a specific emphasis on robustness and generalization capabilities of the methods. Our data set comprises 30 laparoscopic videos and corresponding sensor data from medical devices in the operating room for three different types of laparoscopic surgery. Annotations include surgical phase labels for all frames in the videos as well as instance-wise segmentation masks for surgical instruments in more than 10,000 individual frames. The data has successfully been used to organize international competitions in the scope of the Endoscopic Vision Challenges (EndoVis) 2017 and 2019.
Robust Medical Instrument Segmentation Challenge 2019
Mar 23, 2020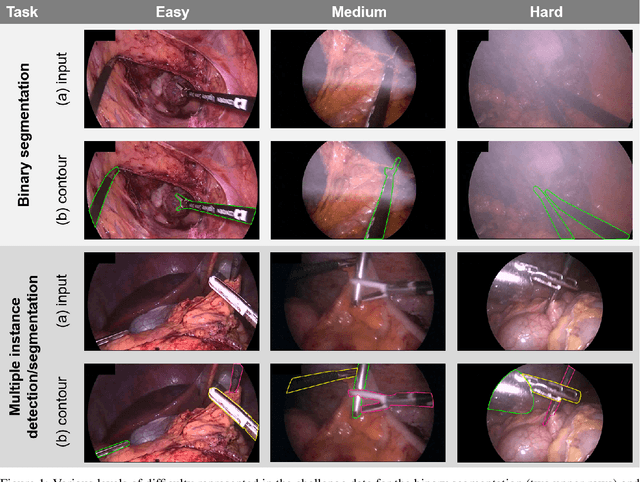
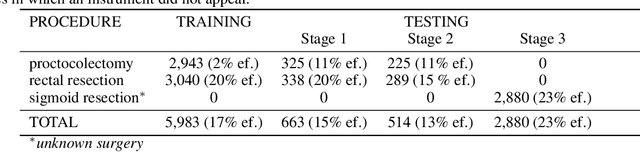
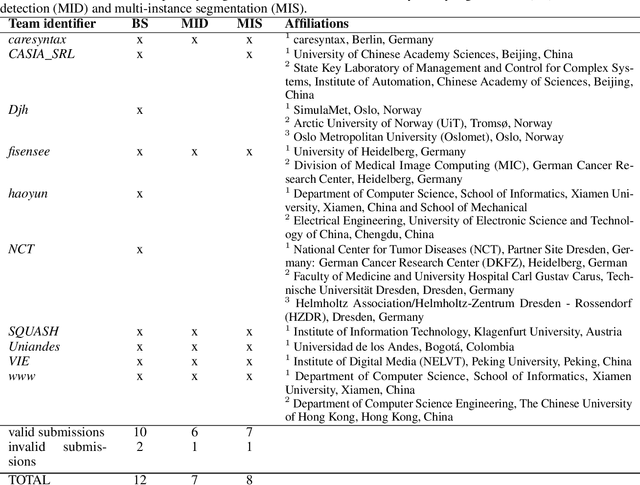
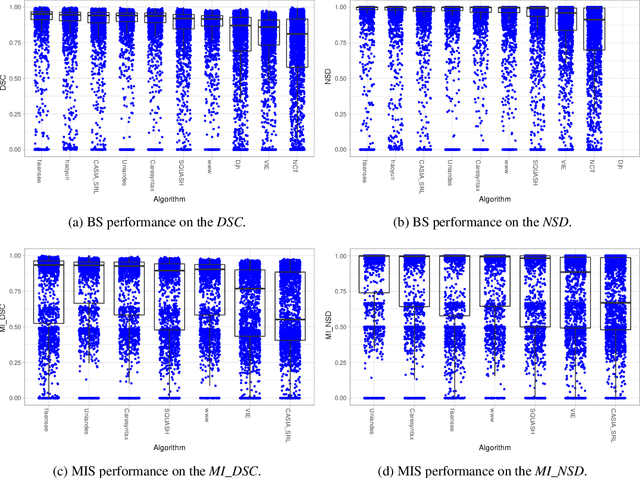
Intraoperative tracking of laparoscopic instruments is often a prerequisite for computer and robotic-assisted interventions. While numerous methods for detecting, segmenting and tracking of medical instruments based on endoscopic video images have been proposed in the literature, key limitations remain to be addressed: Firstly, robustness, that is, the reliable performance of state-of-the-art methods when run on challenging images (e.g. in the presence of blood, smoke or motion artifacts). Secondly, generalization; algorithms trained for a specific intervention in a specific hospital should generalize to other interventions or institutions. In an effort to promote solutions for these limitations, we organized the Robust Medical Instrument Segmentation (ROBUST-MIS) challenge as an international benchmarking competition with a specific focus on the robustness and generalization capabilities of algorithms. For the first time in the field of endoscopic image processing, our challenge included a task on binary segmentation and also addressed multi-instance detection and segmentation. The challenge was based on a surgical data set comprising 10,040 annotated images acquired from a total of 30 surgical procedures from three different types of surgery. The validation of the competing methods for the three tasks (binary segmentation, multi-instance detection and multi-instance segmentation) was performed in three different stages with an increasing domain gap between the training and the test data. The results confirm the initial hypothesis, namely that algorithm performance degrades with an increasing domain gap. While the average detection and segmentation quality of the best-performing algorithms is high, future research should concentrate on detection and segmentation of small, crossing, moving and transparent instrument(s) (parts).
Prediction of laparoscopic procedure duration using unlabeled, multimodal sensor data
Nov 08, 2018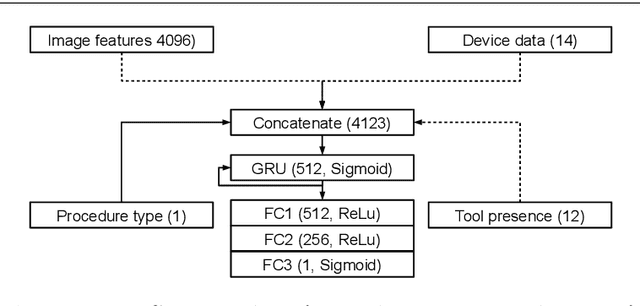
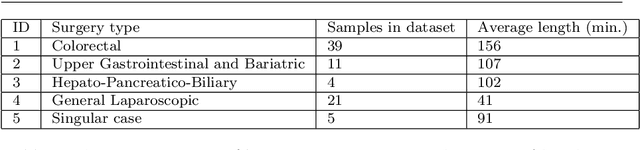
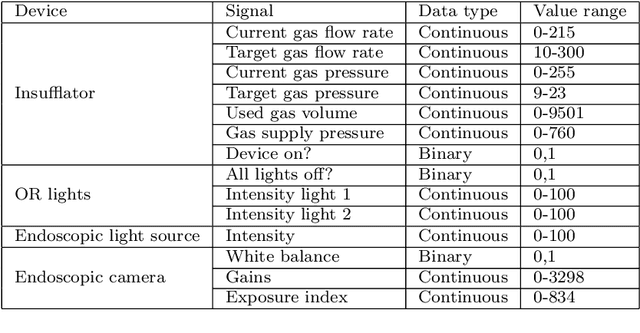
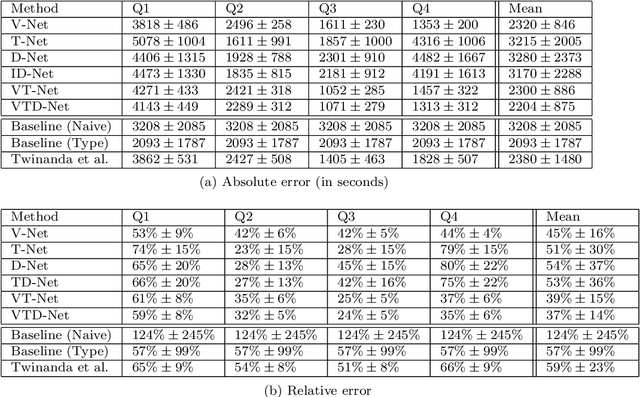
The course of surgical procedures is often unpredictable, making it difficult to estimate the duration of procedures beforehand. This uncertainty makes scheduling surgical procedures a difficult task. A context-aware method that analyses the workflow of an intervention online and automatically predicts the remaining duration would alleviate these problems. As basis for such an estimate, information regarding the current state of the intervention is a requirement. Today, the operating room contains a diverse range of sensors. During laparoscopic interventions, the endoscopic video stream is an ideal source of such information. Extracting quantitative information from the video is challenging though, due to its high dimensionality. Other surgical devices (e.g. insufflator, lights, etc.) provide data streams which are, in contrast to the video stream, more compact and easier to quantify. Though whether such streams offer sufficient information for estimating the duration of surgery is uncertain. In this paper, we propose and compare methods, based on convolutional neural networks, for continuously predicting the duration of laparoscopic interventions based on unlabeled data, such as from endoscopic image and surgical device streams. The methods are evaluated on 80 recorded laparoscopic interventions of various types, for which surgical device data and the endoscopic video streams are available. Here the combined method performs best with an overall average error of 37% and an average halftime error of approximately 28%.
Active Learning using Deep Bayesian Networks for Surgical Workflow Analysis
Nov 08, 2018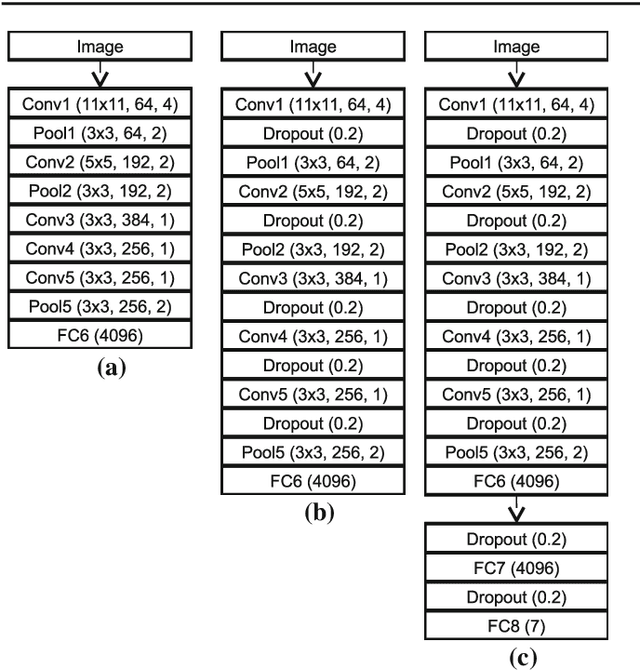

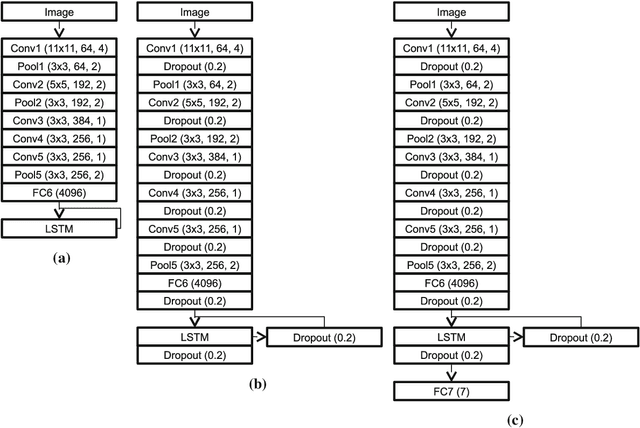
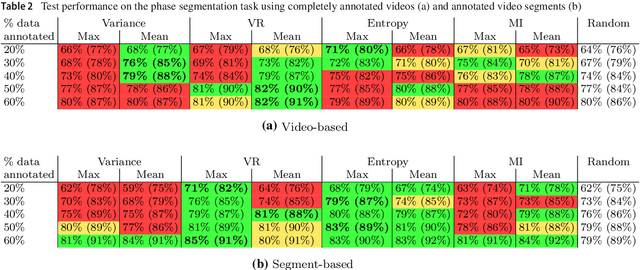
For many applications in the field of computer assisted surgery, such as providing the position of a tumor, specifying the most probable tool required next by the surgeon or determining the remaining duration of surgery, methods for surgical workflow analysis are a prerequisite. Often machine learning based approaches serve as basis for surgical workflow analysis. In general machine learning algorithms, such as convolutional neural networks (CNN), require large amounts of labeled data. While data is often available in abundance, many tasks in surgical workflow analysis need data annotated by domain experts, making it difficult to obtain a sufficient amount of annotations. The aim of using active learning to train a machine learning model is to reduce the annotation effort. Active learning methods determine which unlabeled data points would provide the most information according to some metric, such as prediction uncertainty. Experts will then be asked to only annotate these data points. The model is then retrained with the new data and used to select further data for annotation. Recently, active learning has been applied to CNN by means of Deep Bayesian Networks (DBN). These networks make it possible to assign uncertainties to predictions. In this paper, we present a DBN-based active learning approach adapted for image-based surgical workflow analysis task. Furthermore, by using a recurrent architecture, we extend this network to video-based surgical workflow analysis. We evaluate these approaches on the Cholec80 dataset by performing instrument presence detection and surgical phase segmentation. Here we are able to show that using a DBN-based active learning approach for selecting what data points to annotate next outperforms a baseline based on randomly selecting data points.
Real-time image-based instrument classification for laparoscopic surgery
Aug 01, 2018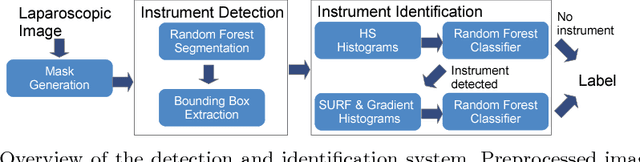


During laparoscopic surgery, context-aware assistance systems aim to alleviate some of the difficulties the surgeon faces. To ensure that the right information is provided at the right time, the current phase of the intervention has to be known. Real-time locating and classification the surgical tools currently in use are key components of both an activity-based phase recognition and assistance generation. In this paper, we present an image-based approach that detects and classifies tools during laparoscopic interventions in real-time. First, potential instrument bounding boxes are detected using a pixel-wise random forest segmentation. Each of these bounding boxes is then classified using a cascade of random forest. For this, multiple features, such as histograms over hue and saturation, gradients and SURF feature, are extracted from each detected bounding box. We evaluated our approach on five different videos from two different types of procedures. We distinguished between the four most common classes of instruments (LigaSure, atraumatic grasper, aspirator, clip applier) and background. Our method succesfully located up to 86% of all instruments respectively. On manually provided bounding boxes, we achieve a instrument type recognition rate of up to 58% and on automatically detected bounding boxes up to 49%. To our knowledge, this is the first approach that allows an image-based classification of surgical tools in a laparoscopic setting in real-time.
* Workshop paper accepted and presented at Modeling and Monitoring of Computer Assisted Interventions (M2CAI) (2015)
Comparative evaluation of instrument segmentation and tracking methods in minimally invasive surgery
May 07, 2018
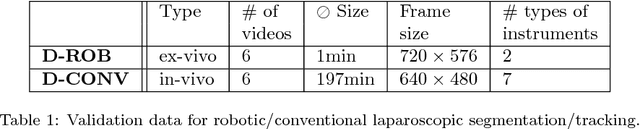

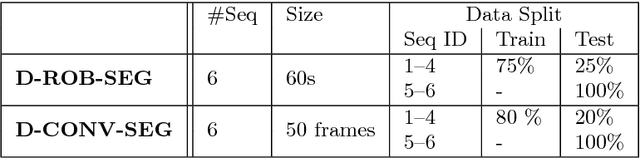
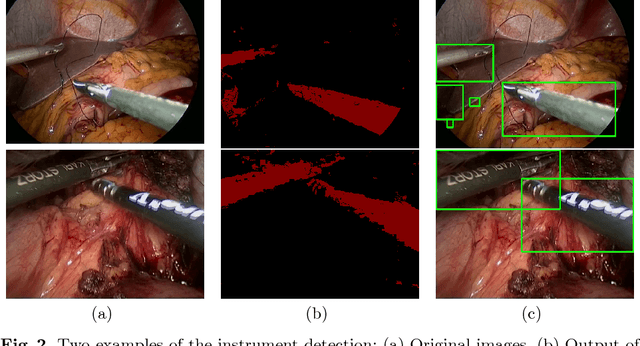
Intraoperative segmentation and tracking of minimally invasive instruments is a prerequisite for computer- and robotic-assisted surgery. Since additional hardware like tracking systems or the robot encoders are cumbersome and lack accuracy, surgical vision is evolving as promising techniques to segment and track the instruments using only the endoscopic images. However, what is missing so far are common image data sets for consistent evaluation and benchmarking of algorithms against each other. The paper presents a comparative validation study of different vision-based methods for instrument segmentation and tracking in the context of robotic as well as conventional laparoscopic surgery. The contribution of the paper is twofold: we introduce a comprehensive validation data set that was provided to the study participants and present the results of the comparative validation study. Based on the results of the validation study, we arrive at the conclusion that modern deep learning approaches outperform other methods in instrument segmentation tasks, but the results are still not perfect. Furthermore, we show that merging results from different methods actually significantly increases accuracy in comparison to the best stand-alone method. On the other hand, the results of the instrument tracking task show that this is still an open challenge, especially during challenging scenarios in conventional laparoscopic surgery.
Exploiting the potential of unlabeled endoscopic video data with self-supervised learning
Jan 31, 2018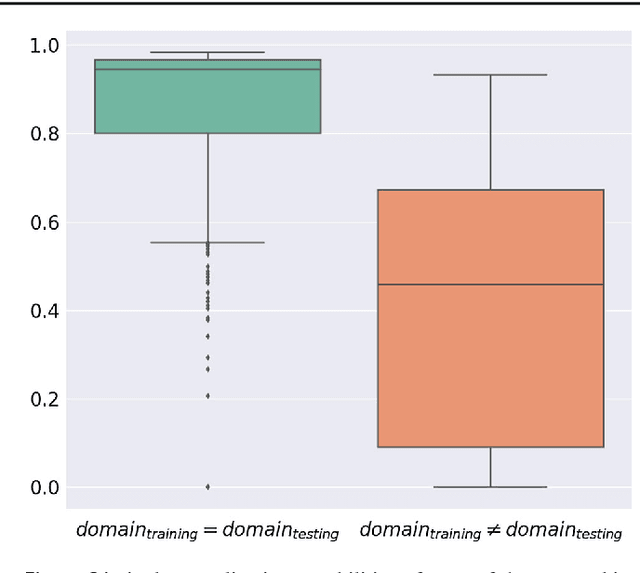
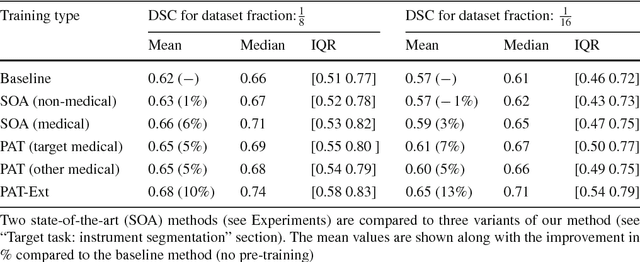
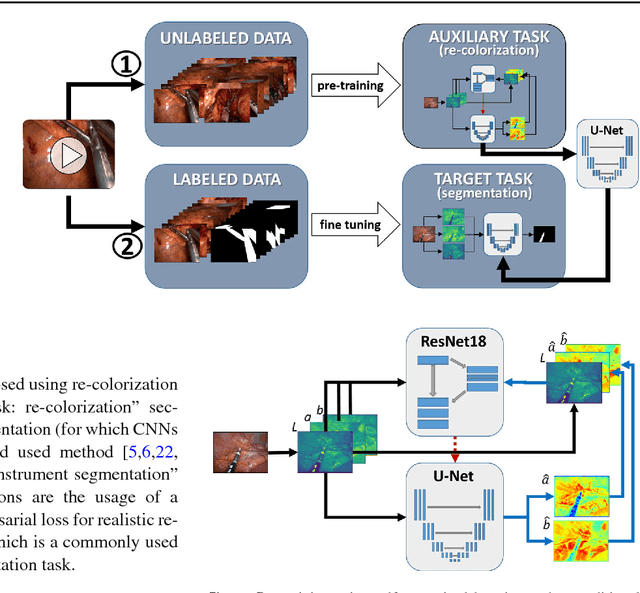
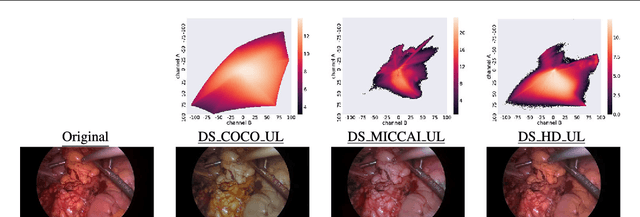
Surgical data science is a new research field that aims to observe all aspects of the patient treatment process in order to provide the right assistance at the right time. Due to the breakthrough successes of deep learning-based solutions for automatic image annotation, the availability of reference annotations for algorithm training is becoming a major bottleneck in the field. The purpose of this paper was to investigate the concept of self-supervised learning to address this issue. Our approach is guided by the hypothesis that unlabeled video data can be used to learn a representation of the target domain that boosts the performance of state-of-the-art machine learning algorithms when used for pre-training. Core of the method is an auxiliary task based on raw endoscopic video data of the target domain that is used to initialize the convolutional neural network (CNN) for the target task. In this paper, we propose the re-colorization of medical images with a generative adversarial network (GAN)-based architecture as auxiliary task. A variant of the method involves a second pre-training step based on labeled data for the target task from a related domain. We validate both variants using medical instrument segmentation as target task. The proposed approach can be used to radically reduce the manual annotation effort involved in training CNNs. Compared to the baseline approach of generating annotated data from scratch, our method decreases exploratively the number of labeled images by up to 75% without sacrificing performance. Our method also outperforms alternative methods for CNN pre-training, such as pre-training on publicly available non-medical or medical data using the target task (in this instance: segmentation). As it makes efficient use of available (non-)public and (un-)labeled data, the approach has the potential to become a valuable tool for CNN (pre-)training.
Unsupervised temporal context learning using convolutional neural networks for laparoscopic workflow analysis
Feb 13, 2017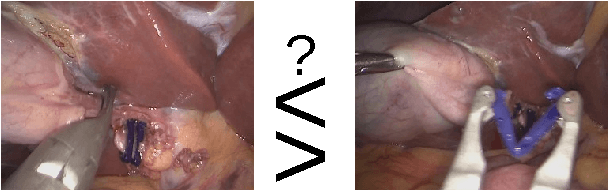
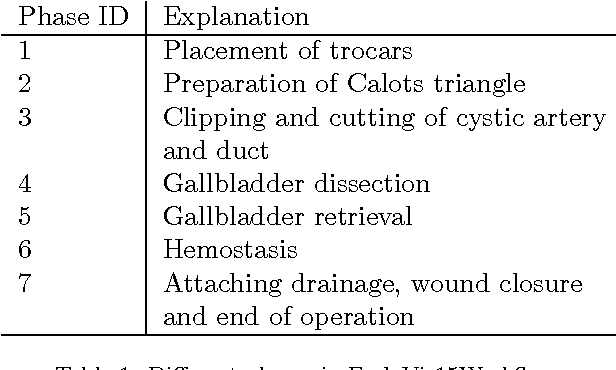
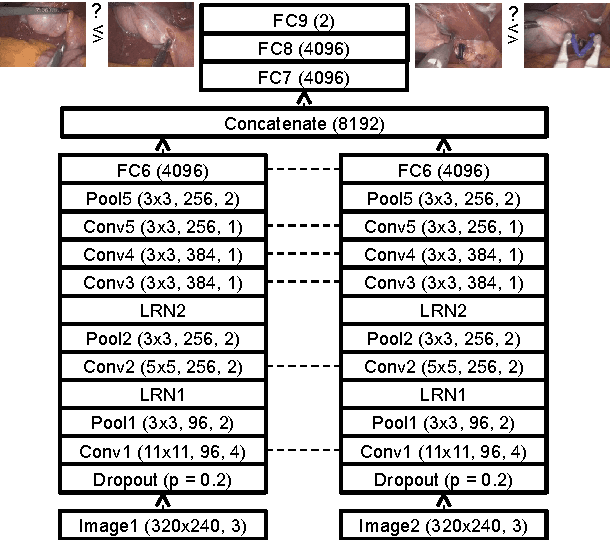
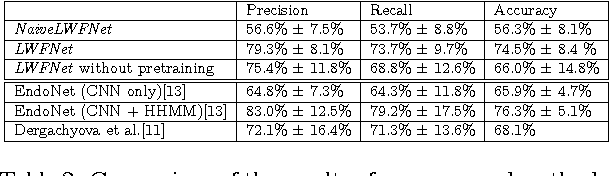
Computer-assisted surgery (CAS) aims to provide the surgeon with the right type of assistance at the right moment. Such assistance systems are especially relevant in laparoscopic surgery, where CAS can alleviate some of the drawbacks that surgeons incur. For many assistance functions, e.g. displaying the location of a tumor at the appropriate time or suggesting what instruments to prepare next, analyzing the surgical workflow is a prerequisite. Since laparoscopic interventions are performed via endoscope, the video signal is an obvious sensor modality to rely on for workflow analysis. Image-based workflow analysis tasks in laparoscopy, such as phase recognition, skill assessment, video indexing or automatic annotation, require a temporal distinction between video frames. Generally computer vision based methods that generalize from previously seen data are used. For training such methods, large amounts of annotated data are necessary. Annotating surgical data requires expert knowledge, therefore collecting a sufficient amount of data is difficult, time-consuming and not always feasible. In this paper, we address this problem by presenting an unsupervised method for training a convolutional neural network (CNN) to differentiate between laparoscopic video frames on a temporal basis. We extract video frames at regular intervals from 324 unlabeled laparoscopic interventions, resulting in a dataset of approximately 2.2 million images. From this dataset, we extract image pairs from the same video and train a CNN to determine their temporal order. To solve this problem, the CNN has to extract features that are relevant for comprehending laparoscopic workflow. Furthermore, we demonstrate that such a CNN can be adapted for surgical workflow segmentation. We performed image-based workflow segmentation on a publicly available dataset of 7 cholecystectomies and 9 colorectal interventions.