 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeJoint Motion Estimation and Segmentation from Undersampled Cardiac MR Image
Aug 20, 2019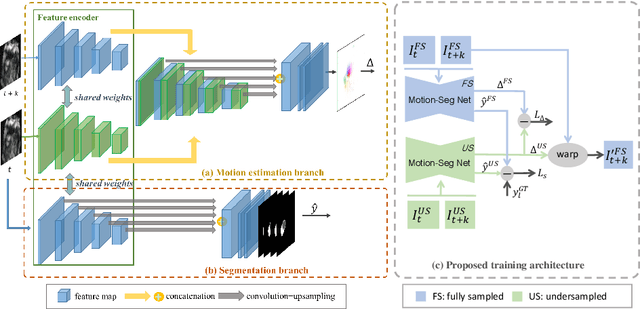
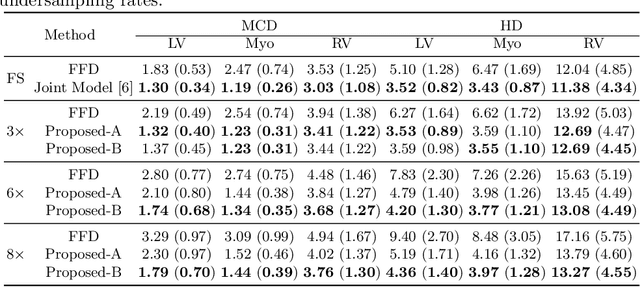
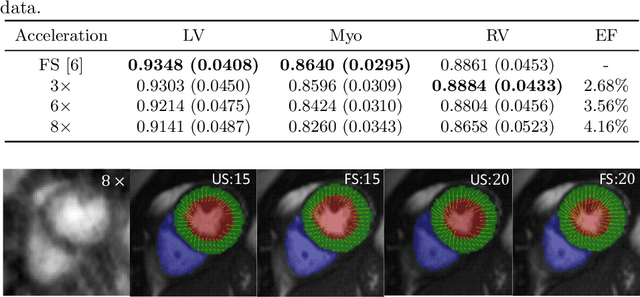
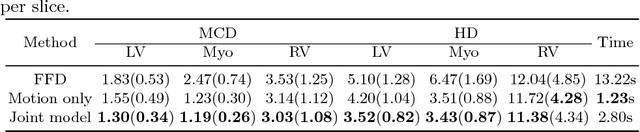
Accelerating the acquisition of magnetic resonance imaging (MRI) is a challenging problem, and many works have been proposed to reconstruct images from undersampled k-space data. However, if the main purpose is to extract certain quantitative measures from the images, perfect reconstructions may not always be necessary as long as the images enable the means of extracting the clinically relevant measures. In this paper, we work on jointly predicting cardiac motion estimation and segmentation directly from undersampled data, which are two important steps in quantitatively assessing cardiac function and diagnosing cardiovascular diseases. In particular, a unified model consisting of both motion estimation branch and segmentation branch is learned by optimising the two tasks simultaneously. Additional corresponding fully-sampled images are incorporated into the network as a parallel sub-network to enhance and guide the learning during the training process. Experimental results using cardiac MR images from 220 subjects show that the proposed model is robust to undersampled data and is capable of predicting results that are close to that from fully-sampled ones, while bypassing the usual image reconstruction stage.
Self-Supervised Learning for Cardiac MR Image Segmentation by Anatomical Position Prediction
Jul 05, 2019
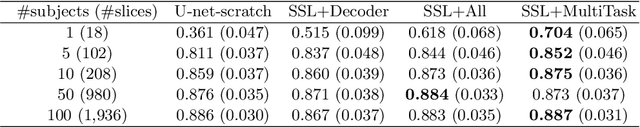

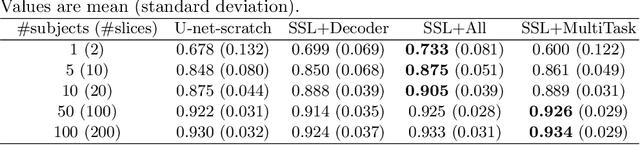
In the recent years, convolutional neural networks have transformed the field of medical image analysis due to their capacity to learn discriminative image features for a variety of classification and regression tasks. However, successfully learning these features requires a large amount of manually annotated data, which is expensive to acquire and limited by the available resources of expert image analysts. Therefore, unsupervised, weakly-supervised and self-supervised feature learning techniques receive a lot of attention, which aim to utilise the vast amount of available data, while at the same time avoid or substantially reduce the effort of manual annotation. In this paper, we propose a novel way for training a cardiac MR image segmentation network, in which features are learnt in a self-supervised manner by predicting anatomical positions. The anatomical positions serve as a supervisory signal and do not require extra manual annotation. We demonstrate that this seemingly simple task provides a strong signal for feature learning and with self-supervised learning, we achieve a high segmentation accuracy that is better than or comparable to a U-net trained from scratch, especially at a small data setting. When only five annotated subjects are available, the proposed method improves the mean Dice metric from 0.811 to 0.852 for short-axis image segmentation, compared to the baseline U-net.
Improving the generalizability of convolutional neural network-based segmentation on CMR images
Jul 03, 2019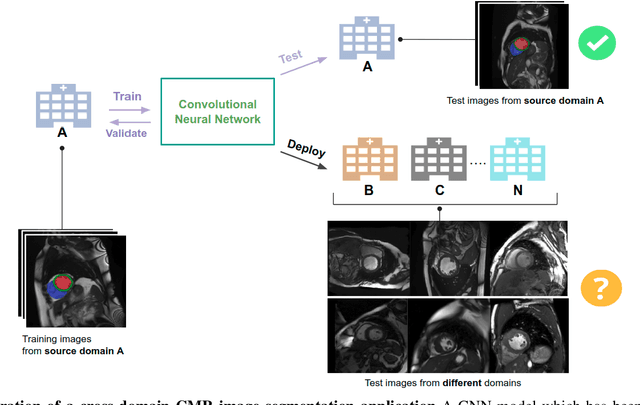
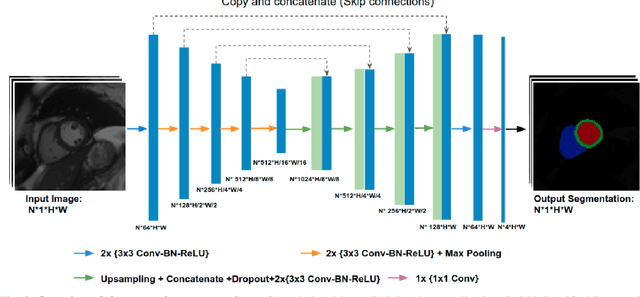
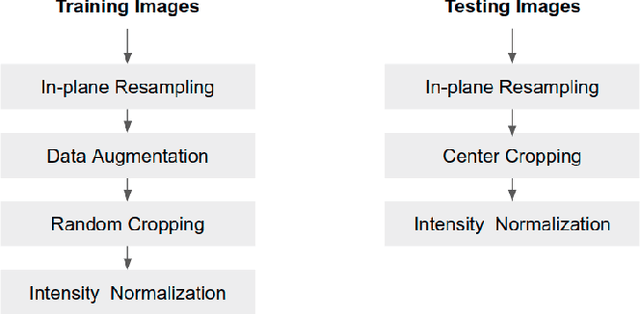
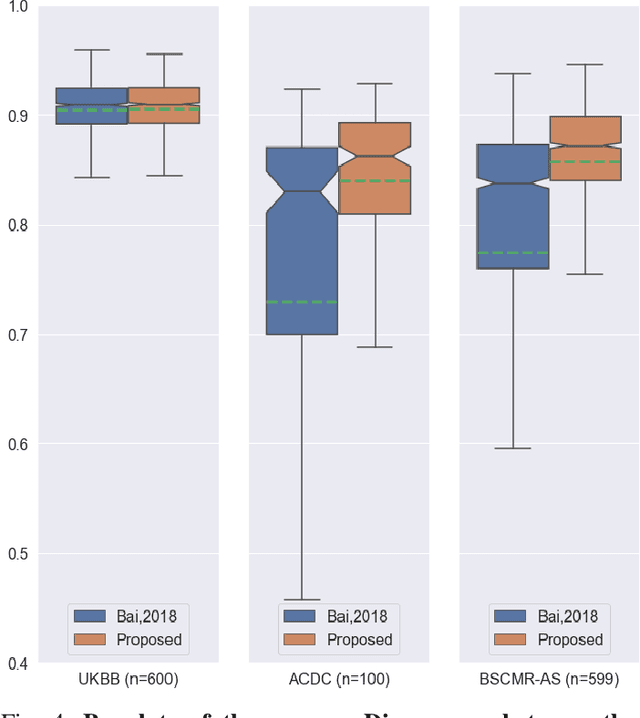
Convolutional neural network (CNN) based segmentation methods provide an efficient and automated way for clinicians to assess the structure and function of the heart in cardiac MR images. While CNNs can generally perform the segmentation tasks with high accuracy when training and test images come from the same domain (e.g. same scanner or site), their performance often degrades dramatically on images from different scanners or clinical sites. We propose a simple yet effective way for improving the network generalization ability by carefully designing data normalization and augmentation strategies to accommodate common scenarios in multi-site, multi-scanner clinical imaging data sets. We demonstrate that a neural network trained on a single-site single-scanner dataset from the UK Biobank can be successfully applied to segmenting cardiac MR images across different sites and different scanners without substantial loss of accuracy. Specifically, the method was trained on a large set of 3,975 subjects from the UK Biobank. It was then directly tested on 600 different subjects from the UK Biobank for intra-domain testing and two other sets for cross-domain testing: the ACDC dataset (100 subjects, 1 site, 2 scanners) and the BSCMR-AS dataset (599 subjects, 6 sites, 9 scanners). The proposed method produces promising segmentation results on the UK Biobank test set which are comparable to previously reported values in the literature, while also performing well on cross-domain test sets, achieving a mean Dice metric of 0.90 for the left ventricle, 0.81 for the myocardium and 0.82 for the right ventricle on the ACDC dataset; and 0.89 for the left ventricle, 0.83 for the myocardium on the BSCMR-AS dataset. The proposed method offers a potential solution to improve CNN-based model generalizability for the cross-scanner and cross-site cardiac MR image segmentation task.
3D Cardiac Shape Prediction with Deep Neural Networks: Simultaneous Use of Images and Patient Metadata
Jul 02, 2019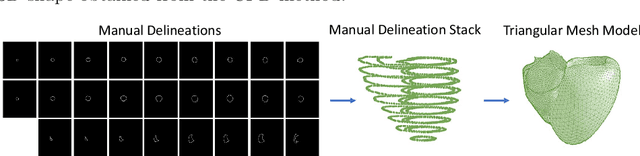
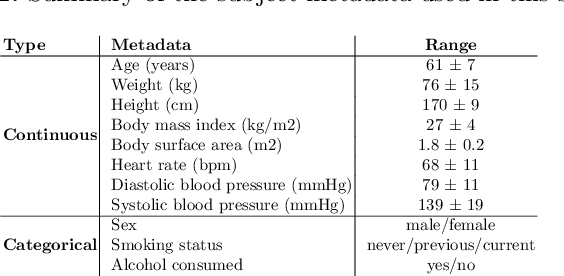
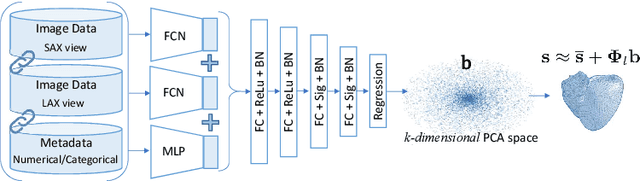

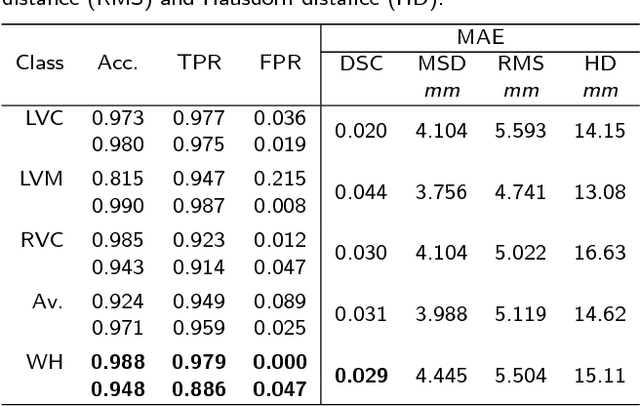
Large prospective epidemiological studies acquire cardiovascular magnetic resonance (CMR) images for pre-symptomatic populations and follow these over time. To support this approach, fully automatic large-scale 3D analysis is essential. In this work, we propose a novel deep neural network using both CMR images and patient metadata to directly predict cardiac shape parameters. The proposed method uses the promising ability of statistical shape models to simplify shape complexity and variability together with the advantages of convolutional neural networks for the extraction of solid visual features. To the best of our knowledge, this is the first work that uses such an approach for 3D cardiac shape prediction. We validated our proposed CMR analytics method against a reference cohort containing 500 3D shapes of the cardiac ventricles. Our results show broadly significant agreement with the reference shapes in terms of the estimated volume of the cardiac ventricles, myocardial mass, 3D Dice, and mean and Hausdorff distance.
Unsupervised shape and motion analysis of 3822 cardiac 4D MRIs of UK Biobank
Feb 15, 2019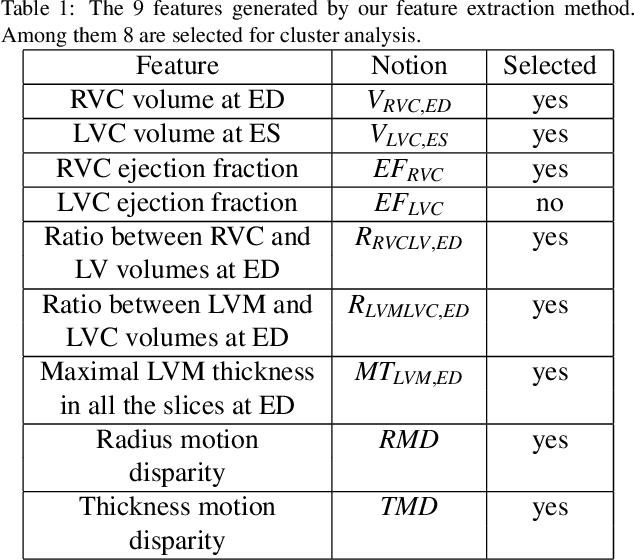
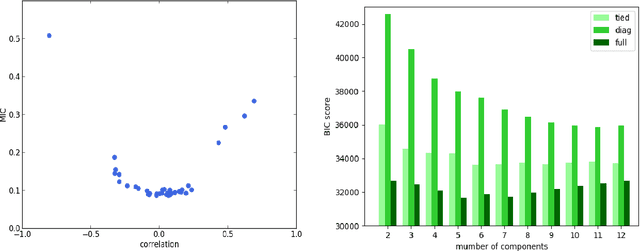
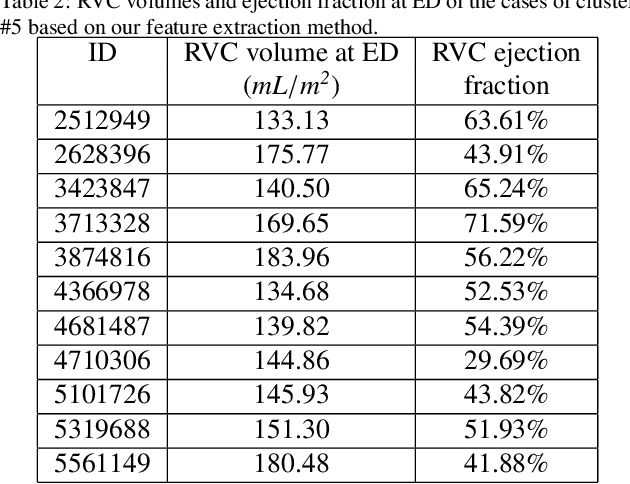
We perform unsupervised analysis of image-derived shape and motion features extracted from 3822 cardiac 4D MRIs of the UK Biobank. First, with a feature extraction method previously published based on deep learning models, we extract from each case 9 feature values characterizing both the cardiac shape and motion. Second, a feature selection is performed to remove highly correlated feature pairs. Third, clustering is carried out using a Gaussian mixture model on the selected features. After analysis, we identify two small clusters which probably correspond to two pathological categories. Further confirmation using a trained classification model and dimensionality reduction tools is carried out to support this discovery. Moreover, we examine the differences between the other large clusters and compare our measures with the ground-truth.
Automated Quality Control in Image Segmentation: Application to the UK Biobank Cardiac MR Imaging Study
Jan 27, 2019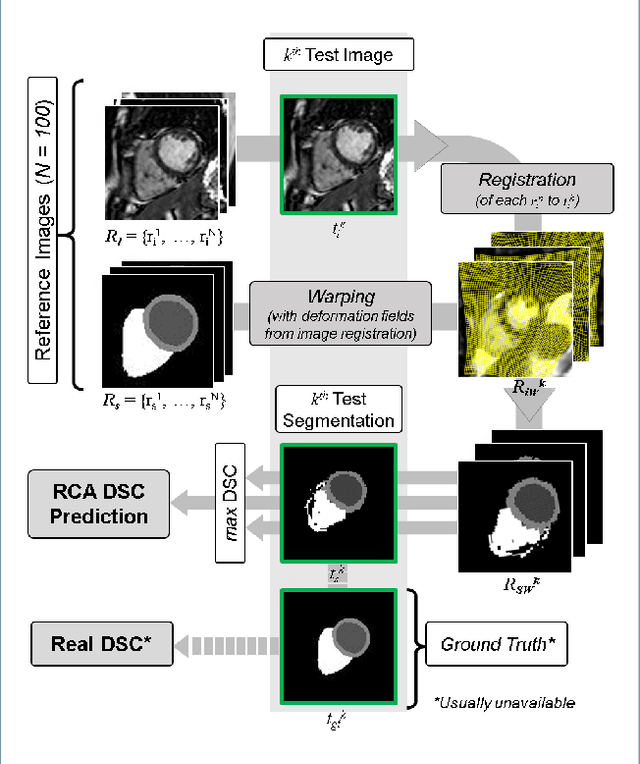
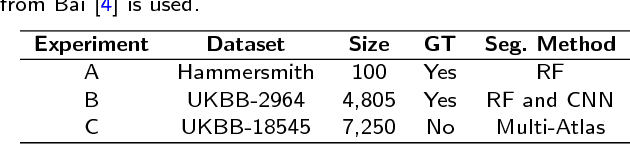
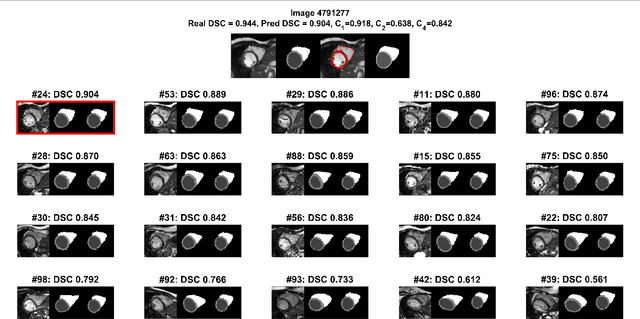
Background: The trend towards large-scale studies including population imaging poses new challenges in terms of quality control (QC). This is a particular issue when automatic processing tools, e.g. image segmentation methods, are employed to derive quantitative measures or biomarkers for later analyses. Manual inspection and visual QC of each segmentation isn't feasible at large scale. However, it's important to be able to automatically detect when a segmentation method fails so as to avoid inclusion of wrong measurements into subsequent analyses which could lead to incorrect conclusions. Methods: To overcome this challenge, we explore an approach for predicting segmentation quality based on Reverse Classification Accuracy, which enables us to discriminate between successful and failed segmentations on a per-cases basis. We validate this approach on a new, large-scale manually-annotated set of 4,800 cardiac magnetic resonance scans. We then apply our method to a large cohort of 7,250 cardiac MRI on which we have performed manual QC. Results: We report results used for predicting segmentation quality metrics including Dice Similarity Coefficient (DSC) and surface-distance measures. As initial validation, we present data for 400 scans demonstrating 99% accuracy for classifying low and high quality segmentations using predicted DSC scores. As further validation we show high correlation between real and predicted scores and 95% classification accuracy on 4,800 scans for which manual segmentations were available. We mimic real-world application of the method on 7,250 cardiac MRI where we show good agreement between predicted quality metrics and manual visual QC scores. Conclusions: We show that RCA has the potential for accurate and fully automatic segmentation QC on a per-case basis in the context of large-scale population imaging as in the UK Biobank Imaging Study.
High Throughput Computation of Reference Ranges of Biventricular Cardiac Function on the UK Biobank Population Cohort
Jan 10, 2019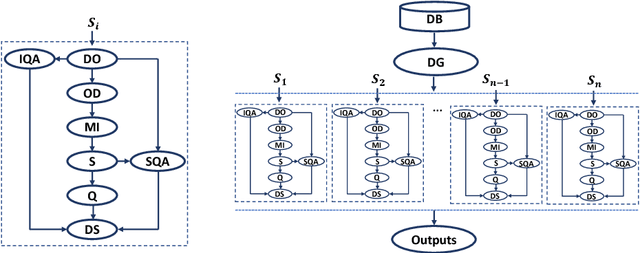
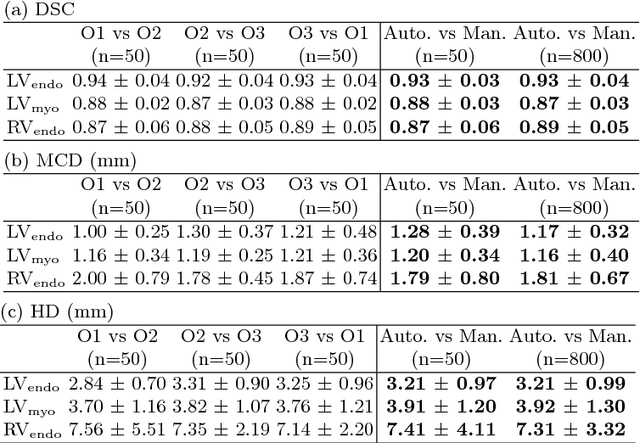

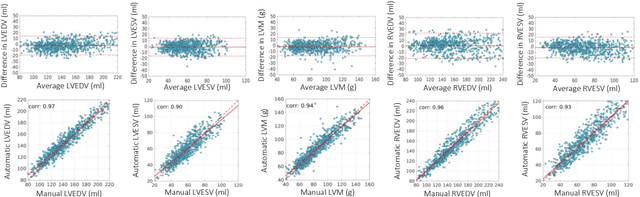
The exploitation of large-scale population data has the potential to improve healthcare by discovering and understanding patterns and trends within this data. To enable high throughput analysis of cardiac imaging data automatically, a pipeline should comprise quality monitoring of the input images, segmentation of the cardiac structures, assessment of the segmentation quality, and parsing of cardiac functional indexes. We present a fully automatic, high throughput image parsing workflow for the analysis of cardiac MR images, and test its performance on the UK Biobank (UKB) cardiac dataset. The proposed pipeline is capable of performing end-to-end image processing including: data organisation, image quality assessment, shape model initialisation, segmentation, segmentation quality assessment, and functional parameter computation; all without any user interaction. To the best of our knowledge,this is the first paper tackling the fully automatic 3D analysis of the UKB population study, providing reference ranges for all key cardiovascular functional indexes, from both left and right ventricles of the heart. We tested our workflow on a reference cohort of 800 healthy subjects for which manual delineations, and reference functional indexes exist. Our results show statistically significant agreement between the manually obtained reference indexes, and those automatically computed using our framework.
Automatic Assessment of Full Left Ventricular Coverage in Cardiac Cine Magnetic Resonance Imaging with Fisher-Discriminative 3D CNN
Nov 08, 2018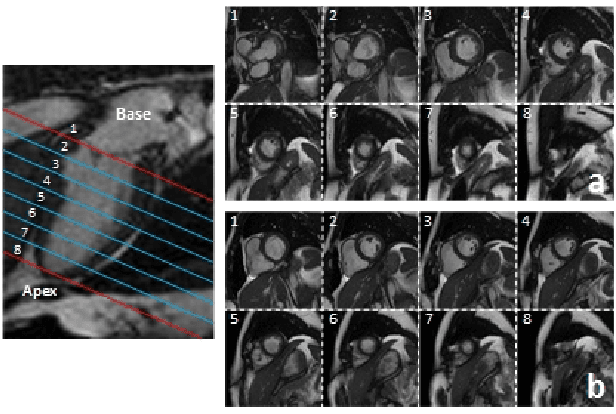
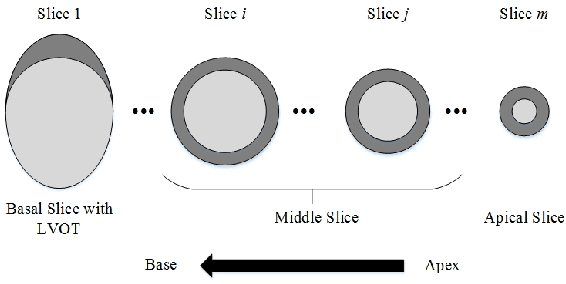
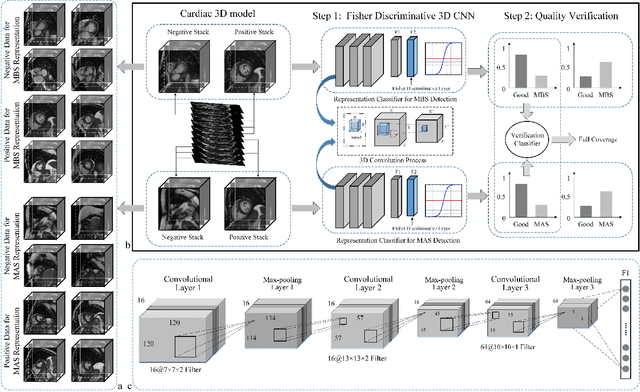
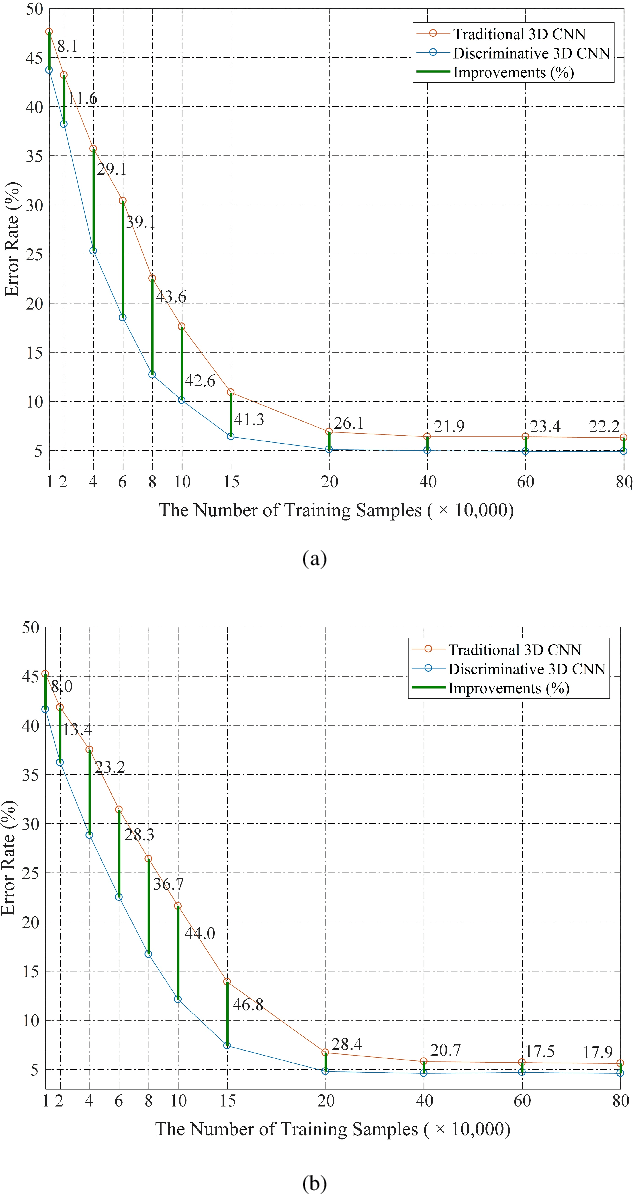
Cardiac magnetic resonance (CMR) images play a growing role in the diagnostic imaging of cardiovascular diseases. Full coverage of the left ventricle (LV), from base to apex, is a basic criterion for CMR image quality and necessary for accurate measurement of cardiac volume and functional assessment. Incomplete coverage of the LV is identified through visual inspection, which is time-consuming and usually done retrospectively in the assessment of large imaging cohorts. This paper proposes a novel automatic method for determining LV coverage from CMR images by using Fisher-discriminative three-dimensional (FD3D) convolutional neural networks (CNNs). In contrast to our previous method employing 2D CNNs, this approach utilizes spatial contextual information in CMR volumes, extracts more representative high-level features and enhances the discriminative capacity of the baseline 2D CNN learning framework, thus achieving superior detection accuracy. A two-stage framework is proposed to identify missing basal and apical slices in measurements of CMR volume. First, the FD3D CNN extracts high-level features from the CMR stacks. These image representations are then used to detect the missing basal and apical slices. Compared to the traditional 3D CNN strategy, the proposed FD3D CNN minimizes within-class scatter and maximizes between-class scatter. We performed extensive experiments to validate the proposed method on more than 5,000 independent volumetric CMR scans from the UK Biobank study, achieving low error rates for missing basal/apical slice detection (4.9\%/4.6\%). The proposed method can also be adopted for assessing LV coverage for other types of CMR image data.
Joint Learning of Motion Estimation and Segmentation for Cardiac MR Image Sequences
Jun 11, 2018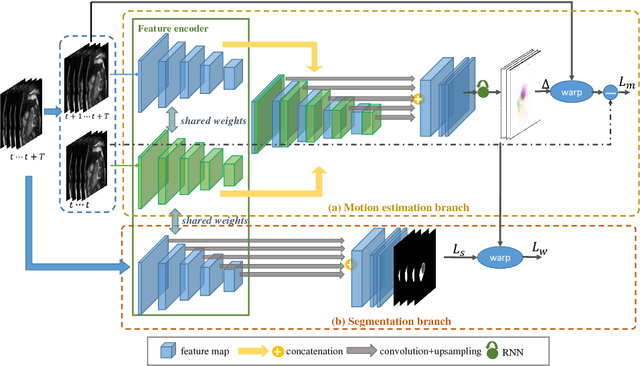

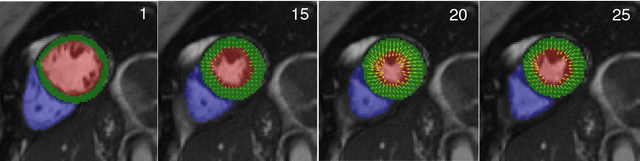
Cardiac motion estimation and segmentation play important roles in quantitatively assessing cardiac function and diagnosing cardiovascular diseases. In this paper, we propose a novel deep learning method for joint estimation of motion and segmentation from cardiac MR image sequences. The proposed network consists of two branches: a cardiac motion estimation branch which is built on a novel unsupervised Siamese style recurrent spatial transformer network, and a cardiac segmentation branch that is based on a fully convolutional network. In particular, a joint multi-scale feature encoder is learned by optimizing the segmentation branch and the motion estimation branch simultaneously. This enables the weakly-supervised segmentation by taking advantage of features that are unsupervisedly learned in the motion estimation branch from a large amount of unannotated data. Experimental results using cardiac MRI images from 220 subjects show that the joint learning of both tasks is complementary and the proposed models outperform the competing methods significantly in terms of accuracy and speed.
Automated cardiovascular magnetic resonance image analysis with fully convolutional networks
May 22, 2018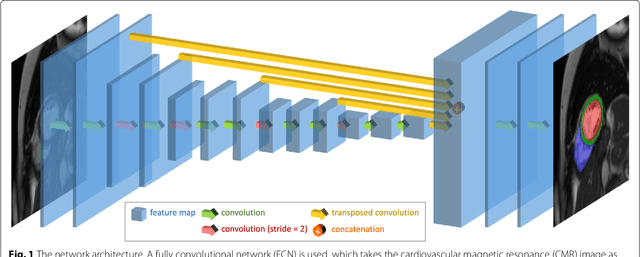
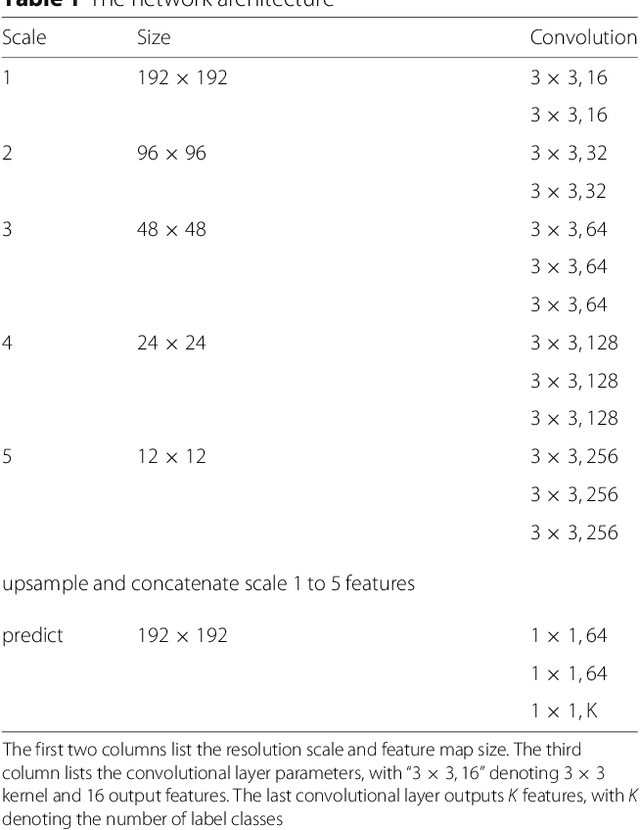
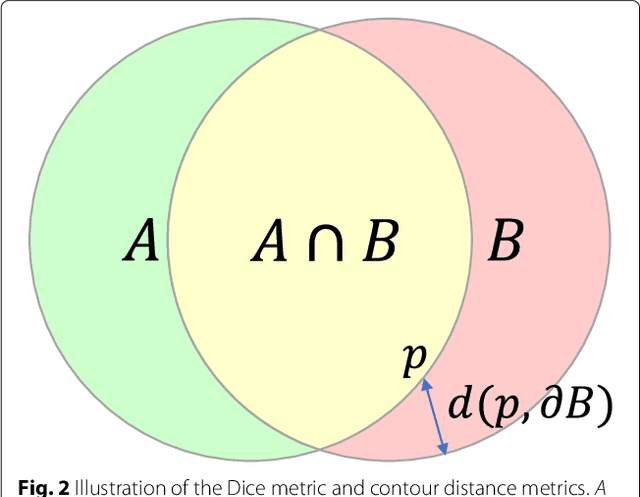
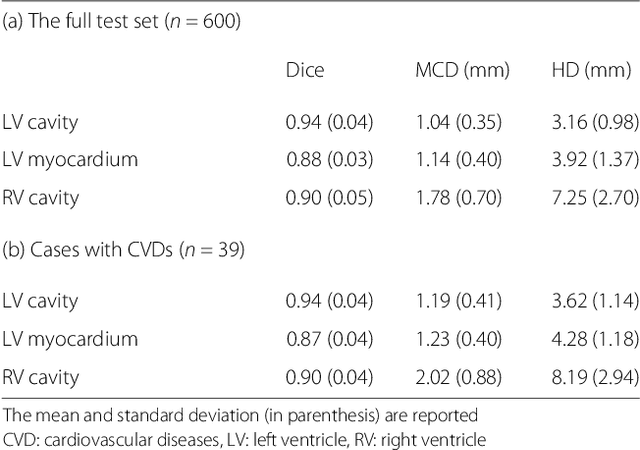
Cardiovascular magnetic resonance (CMR) imaging is a standard imaging modality for assessing cardiovascular diseases (CVDs), the leading cause of death globally. CMR enables accurate quantification of the cardiac chamber volume, ejection fraction and myocardial mass, providing information for diagnosis and monitoring of CVDs. However, for years, clinicians have been relying on manual approaches for CMR image analysis, which is time consuming and prone to subjective errors. It is a major clinical challenge to automatically derive quantitative and clinically relevant information from CMR images. Deep neural networks have shown a great potential in image pattern recognition and segmentation for a variety of tasks. Here we demonstrate an automated analysis method for CMR images, which is based on a fully convolutional network (FCN). The network is trained and evaluated on a large-scale dataset from the UK Biobank, consisting of 4,875 subjects with 93,500 pixelwise annotated images. The performance of the method has been evaluated using a number of technical metrics, including the Dice metric, mean contour distance and Hausdorff distance, as well as clinically relevant measures, including left ventricle (LV) end-diastolic volume (LVEDV) and end-systolic volume (LVESV), LV mass (LVM); right ventricle (RV) end-diastolic volume (RVEDV) and end-systolic volume (RVESV). By combining FCN with a large-scale annotated dataset, the proposed automated method achieves a high performance on par with human experts in segmenting the LV and RV on short-axis CMR images and the left atrium (LA) and right atrium (RA) on long-axis CMR images.