 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeSpeech recognition for medical conversations
Jun 20, 2018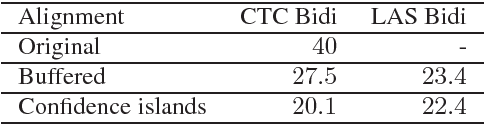
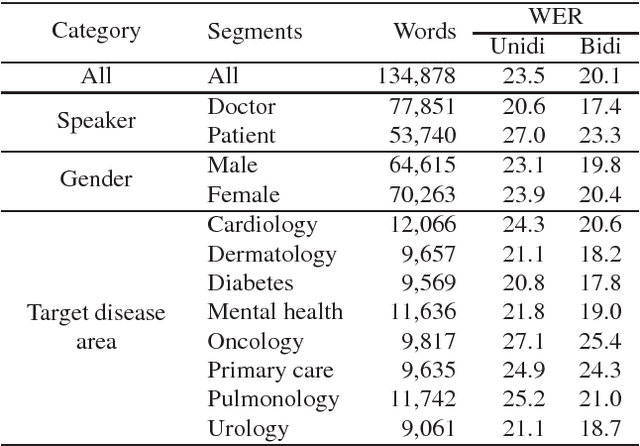
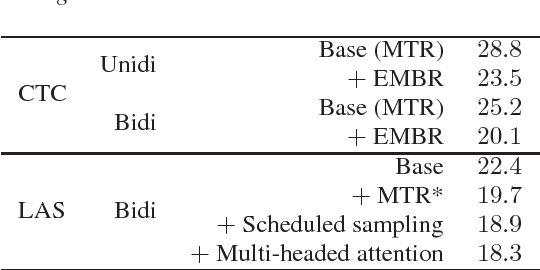
In this work we explored building automatic speech recognition models for transcribing doctor patient conversation. We collected a large scale dataset of clinical conversations ($14,000$ hr), designed the task to represent the real word scenario, and explored several alignment approaches to iteratively improve data quality. We explored both CTC and LAS systems for building speech recognition models. The LAS was more resilient to noisy data and CTC required more data clean up. A detailed analysis is provided for understanding the performance for clinical tasks. Our analysis showed the speech recognition models performed well on important medical utterances, while errors occurred in causal conversations. Overall we believe the resulting models can provide reasonable quality in practice.
Scalable and accurate deep learning for electronic health records
May 11, 2018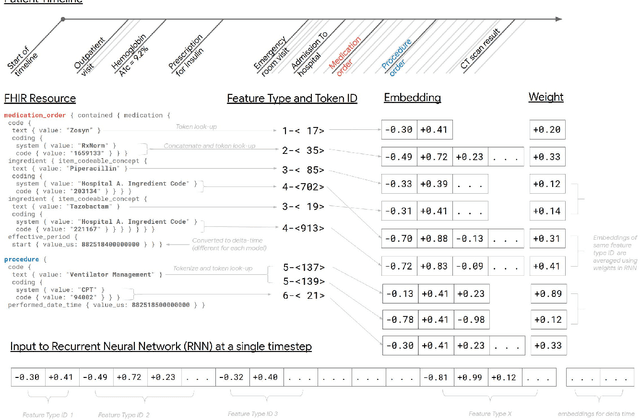
Predictive modeling with electronic health record (EHR) data is anticipated to drive personalized medicine and improve healthcare quality. Constructing predictive statistical models typically requires extraction of curated predictor variables from normalized EHR data, a labor-intensive process that discards the vast majority of information in each patient's record. We propose a representation of patients' entire, raw EHR records based on the Fast Healthcare Interoperability Resources (FHIR) format. We demonstrate that deep learning methods using this representation are capable of accurately predicting multiple medical events from multiple centers without site-specific data harmonization. We validated our approach using de-identified EHR data from two U.S. academic medical centers with 216,221 adult patients hospitalized for at least 24 hours. In the sequential format we propose, this volume of EHR data unrolled into a total of 46,864,534,945 data points, including clinical notes. Deep learning models achieved high accuracy for tasks such as predicting in-hospital mortality (AUROC across sites 0.93-0.94), 30-day unplanned readmission (AUROC 0.75-0.76), prolonged length of stay (AUROC 0.85-0.86), and all of a patient's final discharge diagnoses (frequency-weighted AUROC 0.90). These models outperformed state-of-the-art traditional predictive models in all cases. We also present a case-study of a neural-network attribution system, which illustrates how clinicians can gain some transparency into the predictions. We believe that this approach can be used to create accurate and scalable predictions for a variety of clinical scenarios, complete with explanations that directly highlight evidence in the patient's chart.
* Published version from https://www.nature.com/articles/s41746-018-0029-1