 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDQA: Diagnostic Question Answering for IT Support
Apr 07, 2026Enterprise IT support interactions are fundamentally diagnostic: effective resolution requires iterative evidence gathering from ambiguous user reports to identify an underlying root cause. While retrieval-augmented generation (RAG) provides grounding through historical cases, standard multi-turn RAG systems lack explicit diagnostic state and therefore struggle to accumulate evidence and resolve competing hypotheses across turns. We introduce DQA, a diagnostic question-answering framework that maintains persistent diagnostic state and aggregates retrieved cases at the level of root causes rather than individual documents. DQA combines conversational query rewriting, retrieval aggregation, and state-conditioned response generation to support systematic troubleshooting under enterprise latency and context constraints. We evaluate DQA on 150 anonymized enterprise IT support scenarios using a replay-based protocol. Averaged over three independent runs, DQA achieves a 78.7% success rate under a trajectory-level success criterion, compared to 41.3% for a multi-turn RAG baseline, while reducing average turns from 8.4 to 3.9.
VIGIL: Towards Edge-Extended Agentic AI for Enterprise IT Support
Mar 17, 2026Enterprise IT support is constrained by heterogeneous devices, evolving policies, and long-tail failure modes that are difficult to resolve centrally. We present VIGIL, an edge-extended agentic AI system that deploys desktop-resident agents to perform situated diagnosis, retrieval over enterprise knowledge, and policy-governed remediation directly on user devices with explicit consent and end-to-end observability. In a 10-week pilot of VIGIL's operational loop on 100 resource-constrained endpoints, VIGIL reduces interaction rounds by 39%, achieves at least 4 times faster diagnosis, and supports self-service resolution in 82% of matched cases. Users report excellent usability, high trust, and low cognitive workload across four validated instruments, with qualitative feedback highlighting transparency as critical for trust. Notably, users rated the system higher when no historical matches were available, suggesting on-device diagnosis provides value independent of knowledge base coverage. This pilot establishes safety and observability foundations for fleet-wide continuous improvement.
PPLqa: An Unsupervised Information-Theoretic Quality Metric for Comparing Generative Large Language Models
Nov 22, 2024We propose PPLqa, an easy to compute, language independent, information-theoretic metric to measure the quality of responses of generative Large Language Models (LLMs) in an unsupervised way, without requiring ground truth annotations or human supervision. The method and metric enables users to rank generative language models for quality of responses, so as to make a selection of the best model for a given task. Our single metric assesses LLMs with an approach that subsumes, but is not explicitly based on, coherence and fluency (quality of writing) and relevance and consistency (appropriateness of response) to the query. PPLqa performs as well as other related metrics, and works better with long-form Q\&A. Thus, PPLqa enables bypassing the lengthy annotation process required for ground truth evaluations, and it also correlates well with human and LLM rankings.
Improving language models fine-tuning with representation consistency targets
May 23, 2022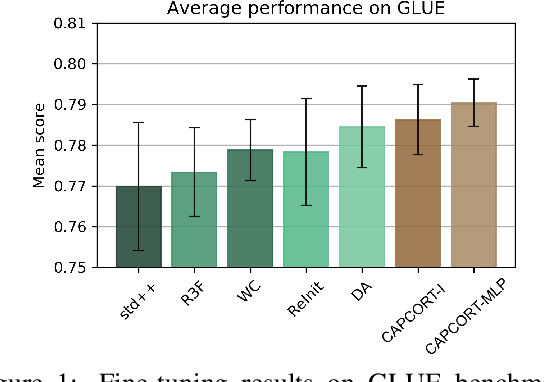
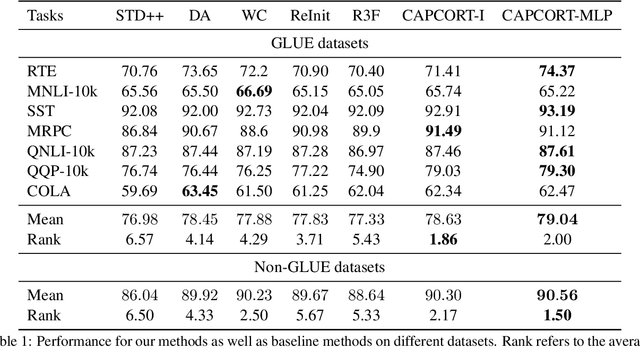
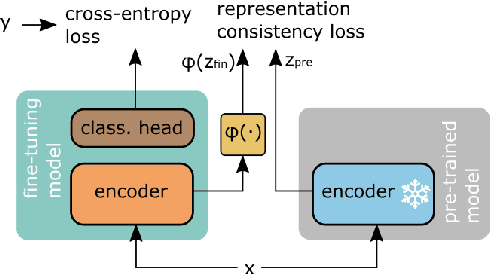
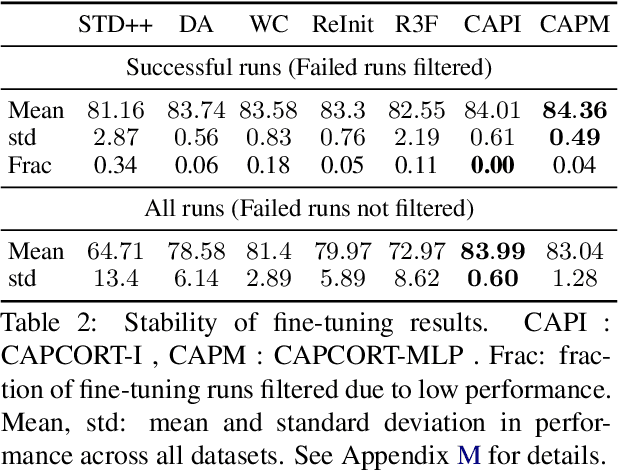
Fine-tuning contextualized representations learned by pre-trained language models has become a standard practice in the NLP field. However, pre-trained representations are prone to degradation (also known as representation collapse) during fine-tuning, which leads to instability, suboptimal performance, and weak generalization. In this paper, we propose a novel fine-tuning method that avoids representation collapse during fine-tuning by discouraging undesirable changes in the representations. We show that our approach matches or exceeds the performance of the existing regularization-based fine-tuning methods across 13 language understanding tasks (GLUE benchmark and six additional datasets). We also demonstrate its effectiveness in low-data settings and robustness to label perturbation. Furthermore, we extend previous studies of representation collapse and propose several metrics to quantify it. Using these metrics and previously proposed experiments, we show that our approach obtains significant improvements in retaining the expressive power of representations.
Improving Early Sepsis Prediction with Multi Modal Learning
Jul 23, 2021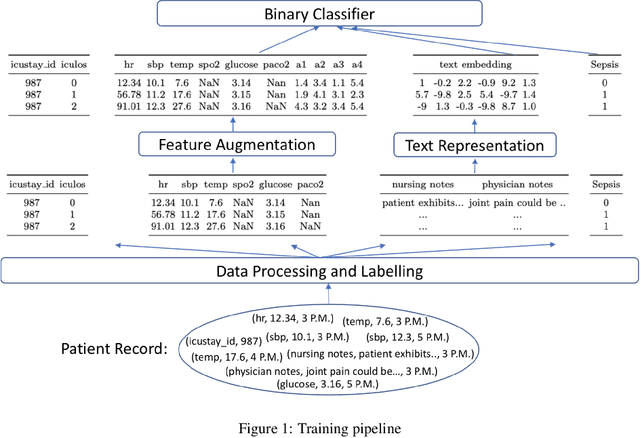
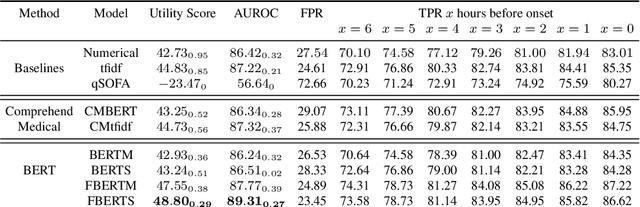
Sepsis is a life-threatening disease with high morbidity, mortality and healthcare costs. The early prediction and administration of antibiotics and intravenous fluids is considered crucial for the treatment of sepsis and can save potentially millions of lives and billions in health care costs. Professional clinical care practitioners have proposed clinical criterion which aid in early detection of sepsis; however, performance of these criterion is often limited. Clinical text provides essential information to estimate the severity of the sepsis in addition to structured clinical data. In this study, we explore how clinical text can complement structured data towards early sepsis prediction task. In this paper, we propose multi modal model which incorporates both structured data in the form of patient measurements as well as textual notes on the patient. We employ state-of-the-art NLP models such as BERT and a highly specialized NLP model in Amazon Comprehend Medical to represent the text. On the MIMIC-III dataset containing records of ICU admissions, we show that by using these notes, one achieves an improvement of 6.07 points in a standard utility score for Sepsis prediction and 2.89% in AUROC score. Our methods significantly outperforms a clinical criteria suggested by experts, qSOFA, as well as the winning model of the PhysioNet Computing in Cardiology Challenge for predicting Sepsis.