 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeVision-language models for chest radiography do not always need the image
Jun 16, 2026Medical vision-language models report strong chest radiograph accuracy, and this is increasingly read as evidence that they use the image. That inference is unsafe: a model exploiting finding-name priors scores like one that reads the scan, and no standard benchmark separates them. We introduce a causal audit that intervenes on the image, occluding the relevant region, occluding an irrelevant one, and swapping in another patient's same-label scan, and combines three behavioral metrics to test whether a correct answer depends on the image. Across nine systems, a text-only model with no image access reaches within 5.7 accuracy points of the best multimodal one, and a 119-billion-parameter multimodal model is statistically indistinguishable from a 7-billion text-only baseline. The audit splits the cohort into three models that ignore the image, one that is unstable, and five that use it selectively, for a subset of findings; the categories hold across a second dataset, resolution, and prompt phrasing. Against board-certified radiologists, a text-only model is statistically indistinguishable from a radiologist's accuracy while grounding at zero, whereas the image-using models ground at radiologist-comparable rates. Reported confidence flags ungrounded answers only when a model uses the image. Grounding audits, not accuracy, should gate clinical deployment.
Routine laboratory trajectories encode the onset of organ-level complications in cancer
Jun 07, 2026Routine laboratory panels drawn during cancer treatment constitute longitudinal physiological recordings of organ function, yet their temporal structure is discarded by single-timepoint prognostic tools. A transformer trained on 2,777,595 laboratory measurements from 3,905 patients with multiple myeloma or ovarian cancer predicted the two-year onset of 162 treatment-associated complications, including therapy-related myelodysplastic syndromes, spanning eight clinical categories, achieving 1.5- to 6.1-fold enrichment above prevalence at the group level. It matched or outperformed non-sequential baselines across grouped endpoints (AUROC gains up to +0.11), demonstrating that longitudinal laboratory trajectories capture evolving complication-specific physiology inaccessible from isolated measurements. Predictions generalised across both cancers, divergence concentrating in disease-specific complications, and biomarker masking recovered signatures consistent with established pathophysiology. External validation on MIMIC-IV and MMRF CoMMpass confirmed transferability across independent healthcare systems (AUROC up to 0.85). Routine oncological laboratory data encode organ deterioration weeks to months before clinical onset, enabling complication-specific surveillance without additional testing infrastructure.
GRASP: Gated Regression-Aware Skill Proposer for Self-Improving LLM Agents
May 28, 2026LLM agents acting in structured environments fail in operational rather than conversational ways, and reliability depends on procedural knowledge of the environment. Prior self-improvement methods accumulate natural-language guidance without checking that each new item preserves previously correct behavior, so a note that fixes one trajectory can silently regress another. We introduce GRASP (Gated Regression-Aware Skill Proposer), which treats agent improvement as a sequence of edits to a bounded skill library, admitting each candidate only if it produces a net improvement on a balanced held-out probe under a hard regression budget. We evaluate GRASP across five base models (gpt-oss-120b, DeepSeek V4 Flash, Gemini 3.1 Flash Lite, GPT-4.1, GPT-5.4) on two FHIR-based clinical benchmarks. On MedAgentBench, GRASP lifts gpt-oss-120b from 40.6% to 88.8%, exceeds the strongest of five self-improvement baselines by 21.0 points, and improves every other base model by 17.2 to 40.3 points. Ablations attribute the gain to comparative proposal generation, the acceptance gate, and the hard regression budget rather than to skill writing itself, which without validation is no better than using no skills. The mechanism generalizes beyond the clinical domain, improving agents on three of four non-clinical environments and remaining flat only where the action space is open-ended. Frozen libraries transfer across models, where skills from a stronger model improve weaker executors beyond what they learn for themselves while the reverse does not, an asymmetry that no ungated baseline reproduces.
Agentic large language models improve retrieval-based radiology question answering
Aug 01, 2025



Clinical decision-making in radiology increasingly benefits from artificial intelligence (AI), particularly through large language models (LLMs). However, traditional retrieval-augmented generation (RAG) systems for radiology question answering (QA) typically rely on single-step retrieval, limiting their ability to handle complex clinical reasoning tasks. Here we propose an agentic RAG framework enabling LLMs to autonomously decompose radiology questions, iteratively retrieve targeted clinical evidence from Radiopaedia, and dynamically synthesize evidence-based responses. We evaluated 24 LLMs spanning diverse architectures, parameter scales (0.5B to >670B), and training paradigms (general-purpose, reasoning-optimized, clinically fine-tuned), using 104 expert-curated radiology questions from previously established RSNA-RadioQA and ExtendedQA datasets. Agentic retrieval significantly improved mean diagnostic accuracy over zero-shot prompting (73% vs. 64%; P<0.001) and conventional online RAG (73% vs. 68%; P<0.001). The greatest gains occurred in mid-sized models (e.g., Mistral Large improved from 72% to 81%) and small-scale models (e.g., Qwen 2.5-7B improved from 55% to 71%), while very large models (>200B parameters) demonstrated minimal changes (<2% improvement). Additionally, agentic retrieval reduced hallucinations (mean 9.4%) and retrieved clinically relevant context in 46% of cases, substantially aiding factual grounding. Even clinically fine-tuned models exhibited meaningful improvements (e.g., MedGemma-27B improved from 71% to 81%), indicating complementary roles of retrieval and fine-tuning. These results highlight the potential of agentic frameworks to enhance factuality and diagnostic accuracy in radiology QA, particularly among mid-sized LLMs, warranting future studies to validate their clinical utility.
LongHealth: A Question Answering Benchmark with Long Clinical Documents
Jan 25, 2024



Background: Recent advancements in large language models (LLMs) offer potential benefits in healthcare, particularly in processing extensive patient records. However, existing benchmarks do not fully assess LLMs' capability in handling real-world, lengthy clinical data. Methods: We present the LongHealth benchmark, comprising 20 detailed fictional patient cases across various diseases, with each case containing 5,090 to 6,754 words. The benchmark challenges LLMs with 400 multiple-choice questions in three categories: information extraction, negation, and sorting, challenging LLMs to extract and interpret information from large clinical documents. Results: We evaluated nine open-source LLMs with a minimum of 16,000 tokens and also included OpenAI's proprietary and cost-efficient GPT-3.5 Turbo for comparison. The highest accuracy was observed for Mixtral-8x7B-Instruct-v0.1, particularly in tasks focused on information retrieval from single and multiple patient documents. However, all models struggled significantly in tasks requiring the identification of missing information, highlighting a critical area for improvement in clinical data interpretation. Conclusion: While LLMs show considerable potential for processing long clinical documents, their current accuracy levels are insufficient for reliable clinical use, especially in scenarios requiring the identification of missing information. The LongHealth benchmark provides a more realistic assessment of LLMs in a healthcare setting and highlights the need for further model refinement for safe and effective clinical application. We make the benchmark and evaluation code publicly available.
From Text to Image: Exploring GPT-4Vision's Potential in Advanced Radiological Analysis across Subspecialties
Nov 24, 2023

The study evaluates and compares GPT-4 and GPT-4Vision for radiological tasks, suggesting GPT-4Vision may recognize radiological features from images, thereby enhancing its diagnostic potential over text-based descriptions.
Comparing Different Deep Learning Architectures for Classification of Chest Radiographs
Feb 20, 2020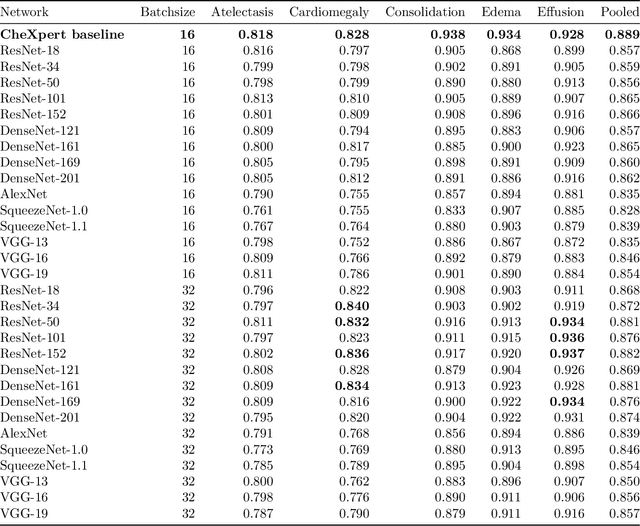
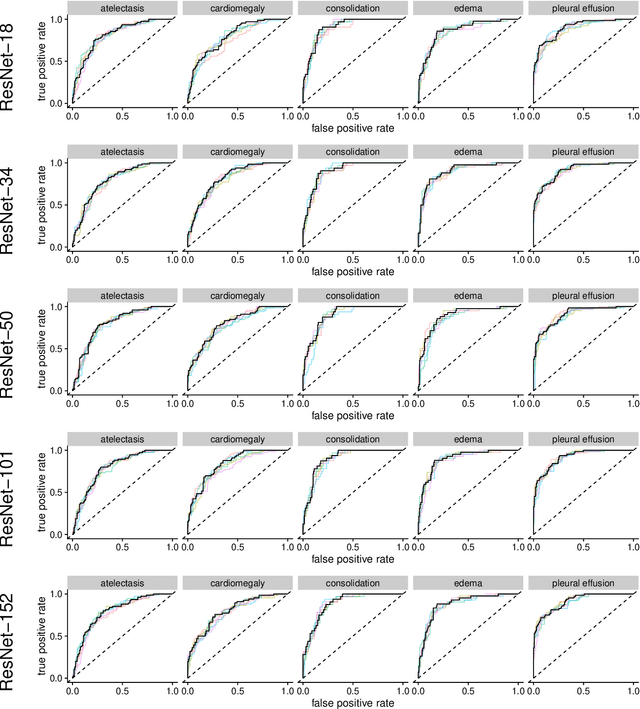
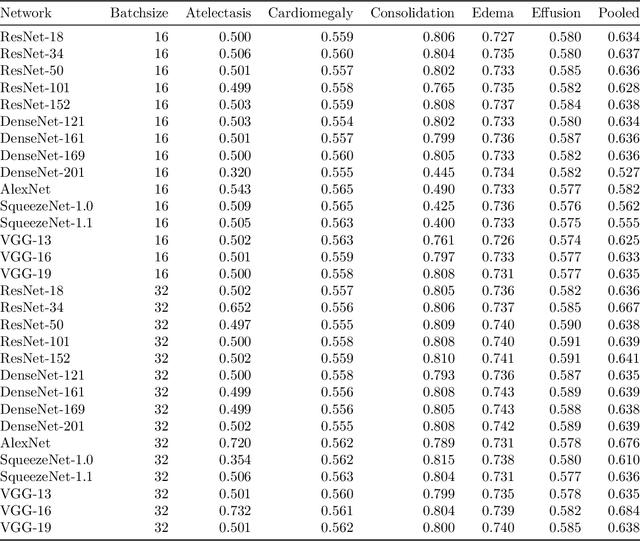
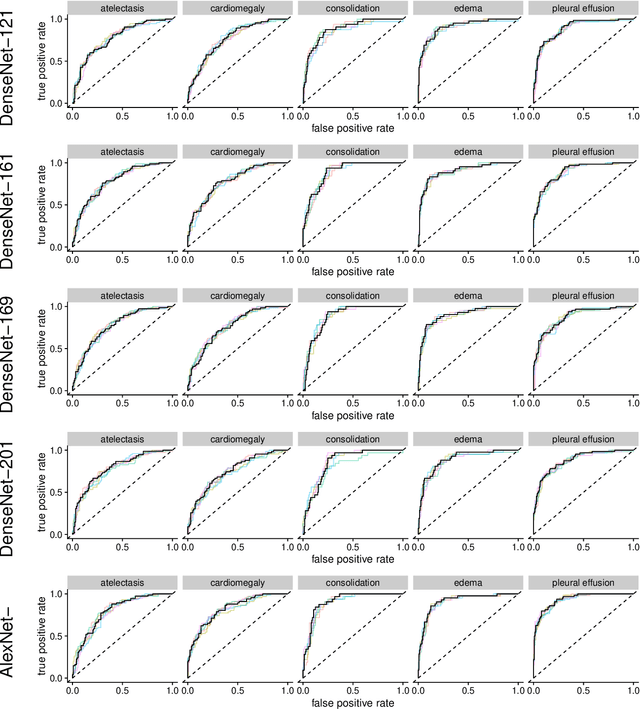
Chest radiographs are among the most frequently acquired images in radiology and are often the subject of computer vision research. However, most of the models used to classify chest radiographs are derived from openly available deep neural networks, trained on large image-datasets. These datasets routinely differ from chest radiographs in that they are mostly color images and contain several possible image classes, while radiographs are greyscale images and often only contain fewer image classes. Therefore, very deep neural networks, which can represent more complex relationships in image-features, might not be required for the comparatively simpler task of classifying grayscale chest radiographs. We compared fifteen different architectures of artificial neural networks regarding training-time and performance on the openly available CheXpert dataset to identify the most suitable models for deep learning tasks on chest radiographs. We could show, that smaller networks such as ResNet-34, AlexNet or VGG-16 have the potential to classify chest radiographs as precisely as deeper neural networks such as DenseNet-201 or ResNet-151, while being less computationally demanding.