 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeText Knows What, Tables Know When: Clinical Timeline Reconstruction via Retrieval-Augmented Multimodal Alignment
May 14, 2026Reconstructing precise clinical timelines is essential for modeling patient trajectories and forecasting risk in complex, heterogeneous conditions like sepsis. While unstructured clinical narratives offer semantically rich and contextually complete descriptions of a patient's course, they often lack temporal precision and contain ambiguous event timing. Conversely, structured electronic health record (EHR) data provides precise temporal anchors but misses a substantial portion of clinically meaningful events. We introduce a retrieval-augmented multimodal alignment framework that bridges this gap to improve the temporal precision of absolute clinical timelines extracted from text. Our approach formulates timeline reconstruction as a graph-based multistep process: it first extracts central anchor events from narratives to build an initial temporal scaffold, places non-central events relative to this backbone, and then calibrates the timeline using retrieved structured EHR rows as external temporal evidence. Evaluated using instruction-tuned large language models on the i2m4 benchmark spanning MIMIC-III and MIMIC-IV, our multimodal pipeline consistently improves absolute timestamp accuracy (AULTC) and improves temporal concordance across nearly all evaluated models over unimodal text-only reconstruction, without compromising event match rates. Furthermore, our empirical gap analysis reveals that 34.8% of text-derived events are entirely absent from tabular records, demonstrating that aligning these modalities can produce a more temporally faithful and clinically informative reconstruction of patient trajectories than either source alone.
Predicting Trajectories of Long COVID in Adult Women: The Critical Role of Causal Disentanglement
Mar 18, 2026Early prediction of Post-Acute Sequelae of SARS-CoV-2 severity is a critical challenge for women's health, particularly given the diagnostic overlap between PASC and common hormonal transitions such as menopause. Identifying and accounting for these confounding factors is essential for accurate long-term trajectory prediction. We conducted a retrospective study of 1,155 women (mean age 61) from the NIH RECOVER dataset. By integrating static clinical profiles with four weeks of longitudinal wearable data (monitoring cardiac activity and sleep), we developed a causal network based on a Large Language Model to predict future PASC scores. Our framework achieved a precision of 86.7\% in clinical severity prediction. Our causal attribution analysis demonstrate the model's ability to differentiate between active pathology and baseline noise: direct indicators such as breathlessness and malaise reached maximum saliency (1.00), while confounding factors like menopause and diabetes were successfully suppressed with saliency scores below 0.27.
SurvHTE-Bench: A Benchmark for Heterogeneous Treatment Effect Estimation in Survival Analysis
Mar 05, 2026Estimating heterogeneous treatment effects (HTEs) from right-censored survival data is critical in high-stakes applications such as precision medicine and individualized policy-making. Yet, the survival analysis setting poses unique challenges for HTE estimation due to censoring, unobserved counterfactuals, and complex identification assumptions. Despite recent advances, from Causal Survival Forests to survival meta-learners and outcome imputation approaches, evaluation practices remain fragmented and inconsistent. We introduce SurvHTE-Bench, the first comprehensive benchmark for HTE estimation with censored outcomes. The benchmark spans (i) a modular suite of synthetic datasets with known ground truth, systematically varying causal assumptions and survival dynamics, (ii) semi-synthetic datasets that pair real-world covariates with simulated treatments and outcomes, and (iii) real-world datasets from a twin study (with known ground truth) and from an HIV clinical trial. Across synthetic, semi-synthetic, and real-world settings, we provide the first rigorous comparison of survival HTE methods under diverse conditions and realistic assumption violations. SurvHTE-Bench establishes a foundation for fair, reproducible, and extensible evaluation of causal survival methods. The data and code of our benchmark are available at: https://github.com/Shahriarnz14/SurvHTE-Bench .
MIMIC-\RNum{4}-Ext-22MCTS: A 22 Millions-Event Temporal Clinical Time-Series Dataset with Relative Timestamp for Risk Prediction
May 01, 2025



Clinical risk prediction based on machine learning algorithms plays a vital role in modern healthcare. A crucial component in developing a reliable prediction model is collecting high-quality time series clinical events. In this work, we release such a dataset that consists of 22,588,586 Clinical Time Series events, which we term MIMIC-\RNum{4}-Ext-22MCTS. Our source data are discharge summaries selected from the well-known yet unstructured MIMIC-IV-Note \cite{Johnson2023-pg}. We then extract clinical events as short text span from the discharge summaries, along with the timestamps of these events as temporal information. The general-purpose MIMIC-IV-Note pose specific challenges for our work: it turns out that the discharge summaries are too lengthy for typical natural language models to process, and the clinical events of interest often are not accompanied with explicit timestamps. Therefore, we propose a new framework that works as follows: 1) we break each discharge summary into manageably small text chunks; 2) we apply contextual BM25 and contextual semantic search to retrieve chunks that have a high potential of containing clinical events; and 3) we carefully design prompts to teach the recently released Llama-3.1-8B \cite{touvron2023llama} model to identify or infer temporal information of the chunks. We show that the obtained dataset is so informative and transparent that standard models fine-tuned on our dataset are achieving significant improvements in healthcare applications. In particular, the BERT model fine-tuned based on our dataset achieves 10\% improvement in accuracy on medical question answering task, and 3\% improvement in clinical trial matching task compared with the classic BERT. The GPT-2 model, fine-tuned on our dataset, produces more clinically reliable results for clinical questions.
Forecasting from Clinical Textual Time Series: Adaptations of the Encoder and Decoder Language Model Families
Apr 14, 2025Clinical case reports encode rich, temporal patient trajectories that are often underexploited by traditional machine learning methods relying on structured data. In this work, we introduce the forecasting problem from textual time series, where timestamped clinical findings--extracted via an LLM-assisted annotation pipeline--serve as the primary input for prediction. We systematically evaluate a diverse suite of models, including fine-tuned decoder-based large language models and encoder-based transformers, on tasks of event occurrence prediction, temporal ordering, and survival analysis. Our experiments reveal that encoder-based models consistently achieve higher F1 scores and superior temporal concordance for short- and long-horizon event forecasting, while fine-tuned masking approaches enhance ranking performance. In contrast, instruction-tuned decoder models demonstrate a relative advantage in survival analysis, especially in early prognosis settings. Our sensitivity analyses further demonstrate the importance of time ordering, which requires clinical time series construction, as compared to text ordering, the format of the text inputs that LLMs are classically trained on. This highlights the additional benefit that can be ascertained from time-ordered corpora, with implications for temporal tasks in the era of widespread LLM use.
Reconstructing Sepsis Trajectories from Clinical Case Reports using LLMs: the Textual Time Series Corpus for Sepsis
Apr 12, 2025



Clinical case reports and discharge summaries may be the most complete and accurate summarization of patient encounters, yet they are finalized, i.e., timestamped after the encounter. Complementary data structured streams become available sooner but suffer from incompleteness. To train models and algorithms on more complete and temporally fine-grained data, we construct a pipeline to phenotype, extract, and annotate time-localized findings within case reports using large language models. We apply our pipeline to generate an open-access textual time series corpus for Sepsis-3 comprising 2,139 case reports from the Pubmed-Open Access (PMOA) Subset. To validate our system, we apply it on PMOA and timeline annotations from I2B2/MIMIC-IV and compare the results to physician-expert annotations. We show high recovery rates of clinical findings (event match rates: O1-preview--0.755, Llama 3.3 70B Instruct--0.753) and strong temporal ordering (concordance: O1-preview--0.932, Llama 3.3 70B Instruct--0.932). Our work characterizes the ability of LLMs to time-localize clinical findings in text, illustrating the limitations of LLM use for temporal reconstruction and providing several potential avenues of improvement via multimodal integration.
Temporal Supervised Contrastive Learning for Modeling Patient Risk Progression
Dec 10, 2023



We consider the problem of predicting how the likelihood of an outcome of interest for a patient changes over time as we observe more of the patient data. To solve this problem, we propose a supervised contrastive learning framework that learns an embedding representation for each time step of a patient time series. Our framework learns the embedding space to have the following properties: (1) nearby points in the embedding space have similar predicted class probabilities, (2) adjacent time steps of the same time series map to nearby points in the embedding space, and (3) time steps with very different raw feature vectors map to far apart regions of the embedding space. To achieve property (3), we employ a nearest neighbor pairing mechanism in the raw feature space. This mechanism also serves as an alternative to data augmentation, a key ingredient of contrastive learning, which lacks a standard procedure that is adequately realistic for clinical tabular data, to our knowledge. We demonstrate that our approach outperforms state-of-the-art baselines in predicting mortality of septic patients (MIMIC-III dataset) and tracking progression of cognitive impairment (ADNI dataset). Our method also consistently recovers the correct synthetic dataset embedding structure across experiments, a feat not achieved by baselines. Our ablation experiments show the pivotal role of our nearest neighbor pairing.
Fair Decision-making Under Uncertainty
Jan 29, 2023



There has been concern within the artificial intelligence (AI) community and the broader society regarding the potential lack of fairness of AI-based decision-making systems. Surprisingly, there is little work quantifying and guaranteeing fairness in the presence of uncertainty which is prevalent in many socially sensitive applications, ranging from marketing analytics to actuarial analysis and recidivism prediction instruments. To this end, we study a longitudinal censored learning problem subject to fairness constraints, where we require that algorithmic decisions made do not affect certain individuals or social groups negatively in the presence of uncertainty on class label due to censorship. We argue that this formulation has a broader applicability to practical scenarios concerning fairness. We show how the newly devised fairness notions involving censored information and the general framework for fair predictions in the presence of censorship allow us to measure and mitigate discrimination under uncertainty that bridges the gap with real-world applications. Empirical evaluations on real-world discriminated datasets with censorship demonstrate the practicality of our approach.
Learning Clinical Concepts for Predicting Risk of Progression to Severe COVID-19
Aug 28, 2022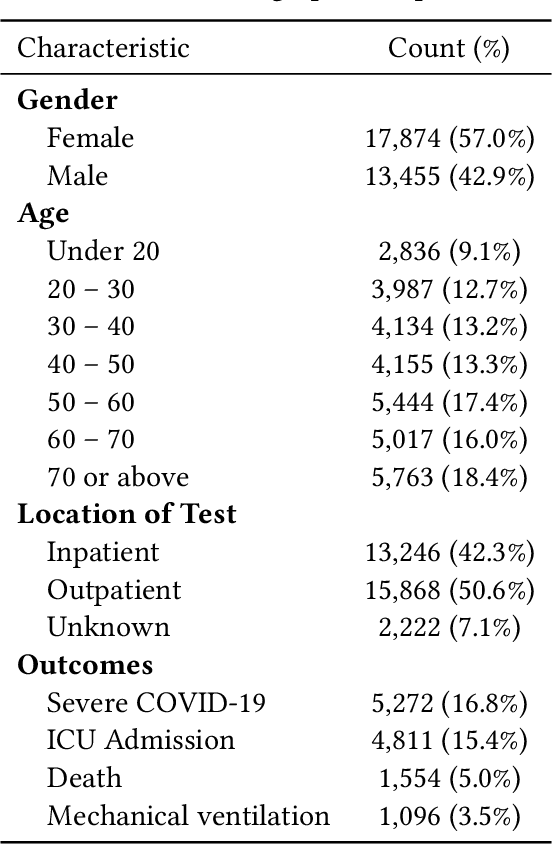
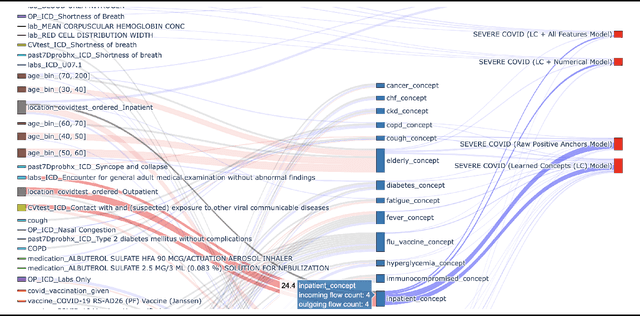
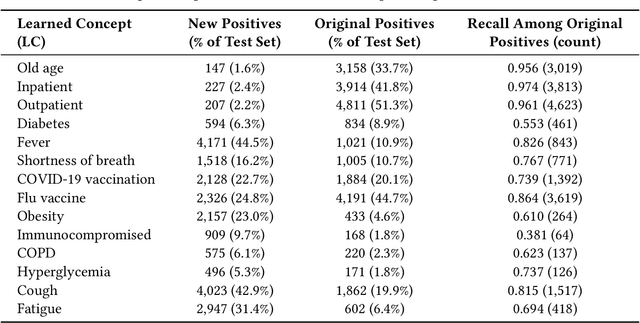
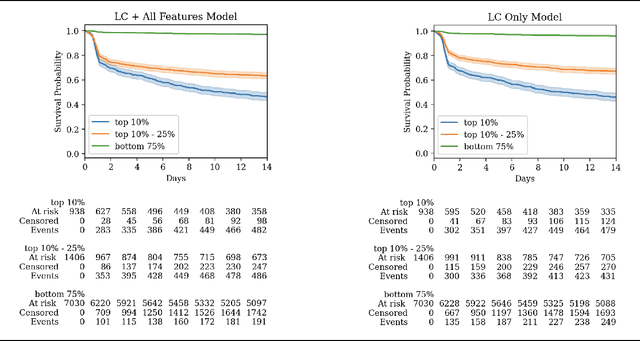
With COVID-19 now pervasive, identification of high-risk individuals is crucial. Using data from a major healthcare provider in Southwestern Pennsylvania, we develop survival models predicting severe COVID-19 progression. In this endeavor, we face a tradeoff between more accurate models relying on many features and less accurate models relying on a few features aligned with clinician intuition. Complicating matters, many EHR features tend to be under-coded, degrading the accuracy of smaller models. In this study, we develop two sets of high-performance risk scores: (i) an unconstrained model built from all available features; and (ii) a pipeline that learns a small set of clinical concepts before training a risk predictor. Learned concepts boost performance over the corresponding features (C-index 0.858 vs. 0.844) and demonstrate improvements over (i) when evaluated out-of-sample (subsequent time periods). Our models outperform previous works (C-index 0.844-0.872 vs. 0.598-0.810).
Longitudinal Fairness with Censorship
Mar 31, 2022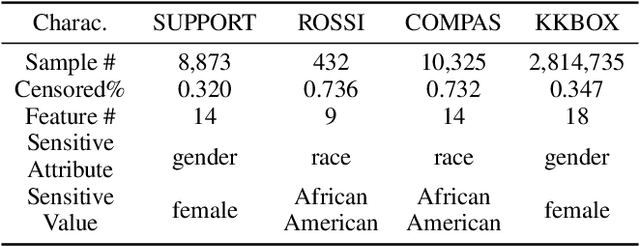
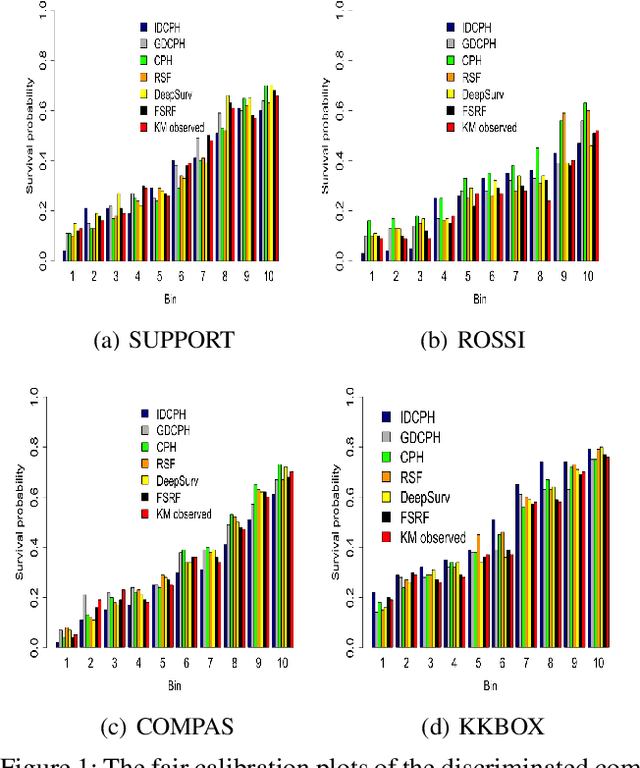
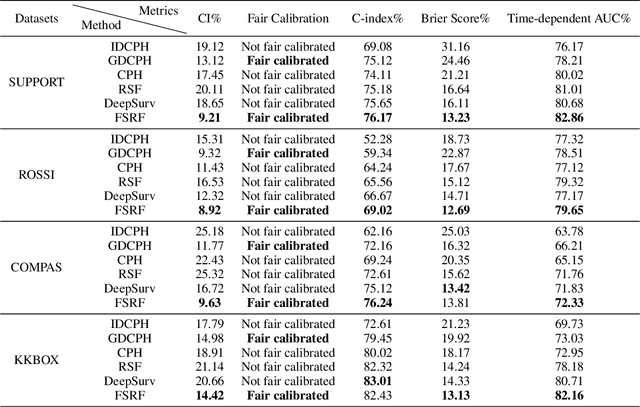

Recent works in artificial intelligence fairness attempt to mitigate discrimination by proposing constrained optimization programs that achieve parity for some fairness statistic. Most assume availability of the class label, which is impractical in many real-world applications such as precision medicine, actuarial analysis and recidivism prediction. Here we consider fairness in longitudinal right-censored environments, where the time to event might be unknown, resulting in censorship of the class label and inapplicability of existing fairness studies. We devise applicable fairness measures, propose a debiasing algorithm, and provide necessary theoretical constructs to bridge fairness with and without censorship for these important and socially-sensitive tasks. Our experiments on four censored datasets confirm the utility of our approach.