 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeRegion of interest detection for efficient aortic segmentation
Jan 13, 2026Thoracic aortic dissection and aneurysms are the most lethal diseases of the aorta. The major hindrance to treatment lies in the accurate analysis of the medical images. More particularly, aortic segmentation of the 3D image is often tedious and difficult. Deep-learning-based segmentation models are an ideal solution, but their inability to deliver usable outputs in difficult cases and their computational cost cause their clinical adoption to stay limited. This study presents an innovative approach for efficient aortic segmentation using targeted region of interest (ROI) detection. In contrast to classical detection models, we propose a simple and efficient detection model that can be widely applied to detect a single ROI. Our detection model is trained as a multi-task model, using an encoder-decoder architecture for segmentation and a fully connected network attached to the bottleneck for detection. We compare the performance of a one-step segmentation model applied to a complete image, nnU-Net and our cascade model composed of a detection and a segmentation step. We achieve a mean Dice similarity coefficient of 0.944 with over 0.9 for all cases using a third of the computing power. This simple solution achieves state-of-the-art performance while being compact and robust, making it an ideal solution for clinical applications.
Learning from Anatomy: Supervised Anatomical Pretraining (SAP) for Improved Metastatic Bone Disease Segmentation in Whole-Body MRI
Jun 24, 2025The segmentation of metastatic bone disease (MBD) in whole-body MRI (WB-MRI) is a challenging problem. Due to varying appearances and anatomical locations of lesions, ambiguous boundaries, and severe class imbalance, obtaining reliable segmentations requires large, well-annotated datasets capturing lesion variability. Generating such datasets requires substantial time and expertise, and is prone to error. While self-supervised learning (SSL) can leverage large unlabeled datasets, learned generic representations often fail to capture the nuanced features needed for accurate lesion detection. In this work, we propose a Supervised Anatomical Pretraining (SAP) method that learns from a limited dataset of anatomical labels. First, an MRI-based skeletal segmentation model is developed and trained on WB-MRI scans from healthy individuals for high-quality skeletal delineation. Then, we compare its downstream efficacy in segmenting MBD on a cohort of 44 patients with metastatic prostate cancer, against both a baseline random initialization and a state-of-the-art SSL method. SAP significantly outperforms both the baseline and SSL-pretrained models, achieving a normalized surface Dice of 0.76 and a Dice coefficient of 0.64. The method achieved a lesion detection F2 score of 0.44, improving on 0.24 (baseline) and 0.31 (SSL). When considering only clinically relevant lesions larger than 1~ml, SAP achieves a detection sensitivity of 100% in 28 out of 32 patients. Learning bone morphology from anatomy yields an effective and domain-relevant inductive bias that can be leveraged for the downstream segmentation task of bone lesions. All code and models are made publicly available.
The STOIC2021 COVID-19 AI challenge: applying reusable training methodologies to private data
Jun 25, 2023Challenges drive the state-of-the-art of automated medical image analysis. The quantity of public training data that they provide can limit the performance of their solutions. Public access to the training methodology for these solutions remains absent. This study implements the Type Three (T3) challenge format, which allows for training solutions on private data and guarantees reusable training methodologies. With T3, challenge organizers train a codebase provided by the participants on sequestered training data. T3 was implemented in the STOIC2021 challenge, with the goal of predicting from a computed tomography (CT) scan whether subjects had a severe COVID-19 infection, defined as intubation or death within one month. STOIC2021 consisted of a Qualification phase, where participants developed challenge solutions using 2000 publicly available CT scans, and a Final phase, where participants submitted their training methodologies with which solutions were trained on CT scans of 9724 subjects. The organizers successfully trained six of the eight Final phase submissions. The submitted codebases for training and running inference were released publicly. The winning solution obtained an area under the receiver operating characteristic curve for discerning between severe and non-severe COVID-19 of 0.815. The Final phase solutions of all finalists improved upon their Qualification phase solutions.HSUXJM-TNZF9CHSUXJM-TNZF9C
Explainable-by-design Semi-Supervised Representation Learning for COVID-19 Diagnosis from CT Imaging
Dec 02, 2020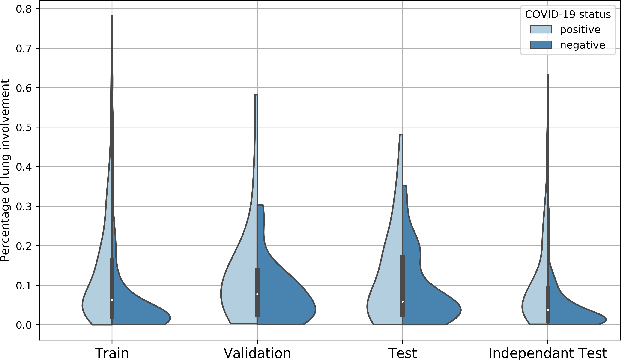
Our motivating application is a real-world problem: COVID-19 classification from CT imaging, for which we present an explainable Deep Learning approach based on a semi-supervised classification pipeline that employs variational autoencoders to extract efficient feature embedding. We have optimized the architecture of two different networks for CT images: (i) a novel conditional variational autoencoder (CVAE) with a specific architecture that integrates the class labels inside the encoder layers and uses side information with shared attention layers for the encoder, which make the most of the contextual clues for representation learning, and (ii) a downstream convolutional neural network for supervised classification using the encoder structure of the CVAE. With the explainable classification results, the proposed diagnosis system is very effective for COVID-19 classification. Based on the promising results obtained qualitatively and quantitatively, we envisage a wide deployment of our developed technique in large-scale clinical studies.Code is available at https://git.etrovub.be/AVSP/ct-based-covid-19-diagnostic-tool.git.
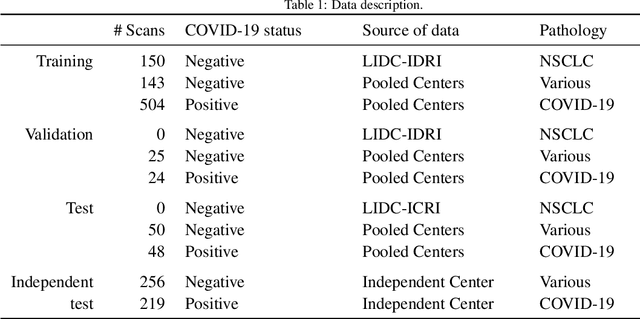
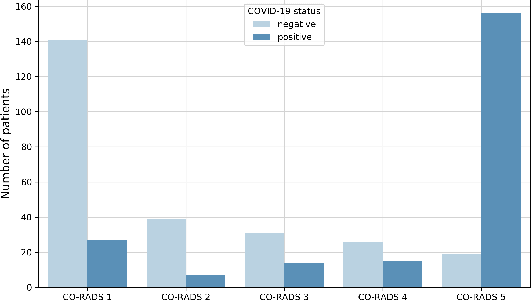
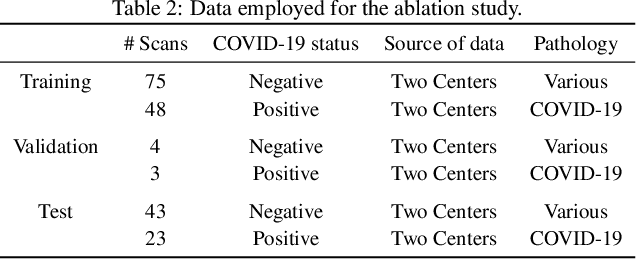
Comparative study of deep learning methods for the automatic segmentation of lung, lesion and lesion type in CT scans of COVID-19 patients
Aug 21, 2020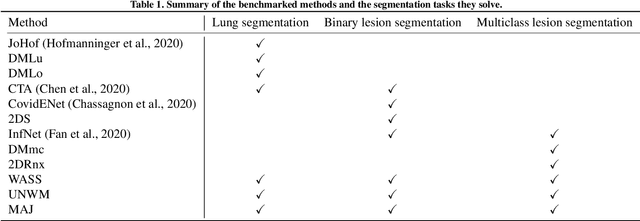
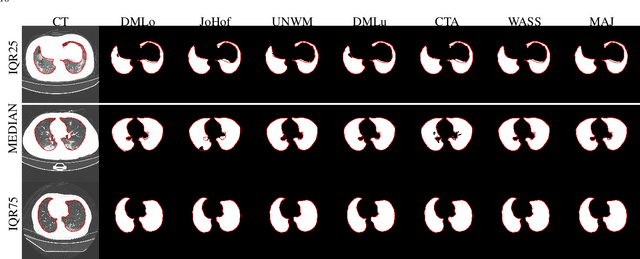
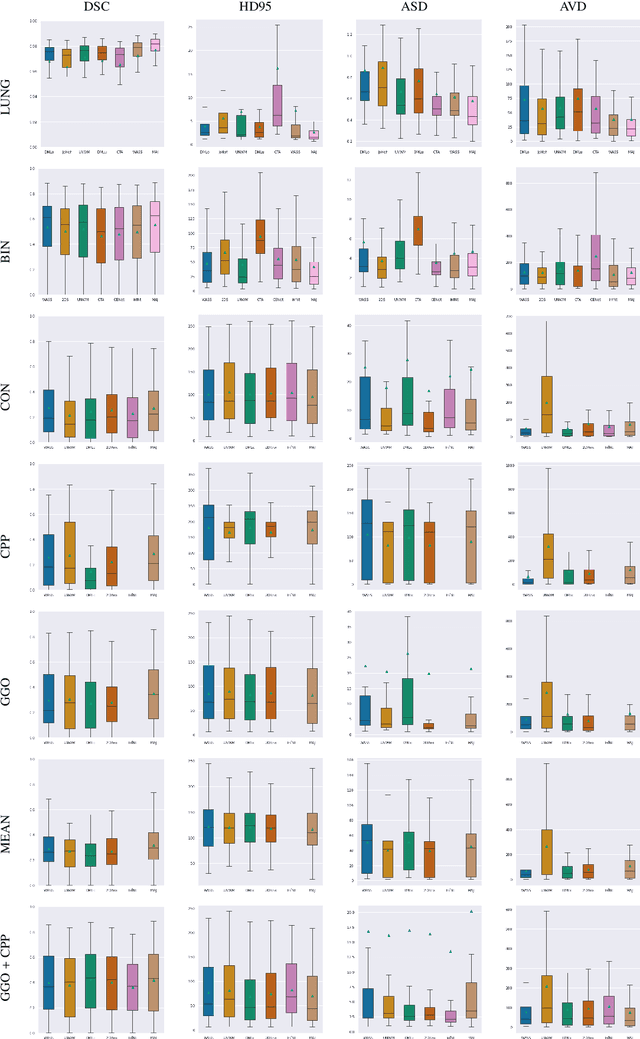
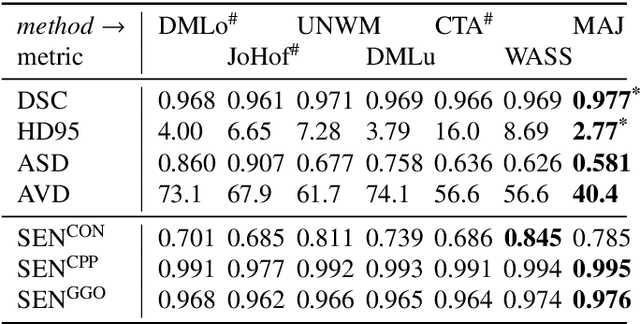
Recent research on COVID-19 suggests that CT imaging provides useful information to assess disease progression and assist diagnosis, in addition to help understanding the disease. There is an increasing number of studies that propose to use deep learning to provide fast and accurate quantification of COVID-19 using chest CT scans. The main tasks of interest are the automatic segmentation of lung and lung lesions in chest CT scans of confirmed or suspected COVID-19 patients. In this study, we compare twelve deep learning algorithms using a multi-center dataset, including both open-source and in-house developed algorithms. Results show that ensembling different methods can boost the overall test set performance for lung segmentation, binary lesion segmentation and multiclass lesion segmentation, resulting in mean Dice scores of 0.982, 0.724 and 0.469, respectively. The resulting binary lesions were segmented with a mean absolute volume error of 91.3 ml. In general, the task of distinguishing different lesion types was more difficult, with a mean absolute volume difference of 152 ml and mean Dice scores of 0.369 and 0.523 for consolidation and ground glass opacity, respectively. All methods perform binary lesion segmentation with an average volume error that is better than visual assessment by human raters, suggesting these methods are mature enough for a large-scale evaluation for use in clinical practice.
Validation, comparison, and combination of algorithms for automatic detection of pulmonary nodules in computed tomography images: the LUNA16 challenge
Jul 15, 2017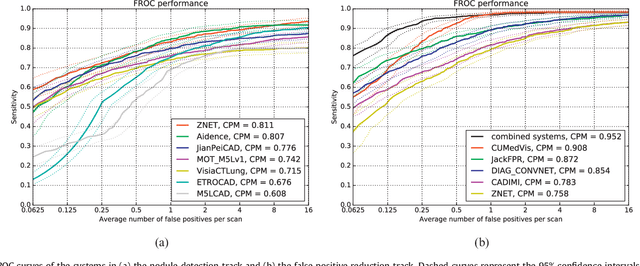
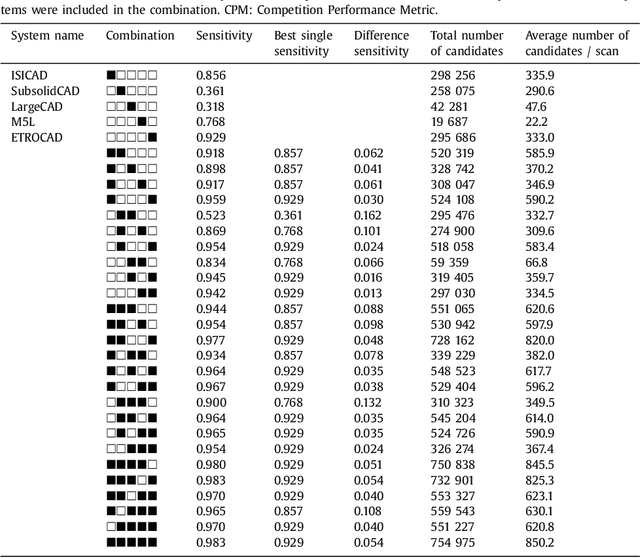
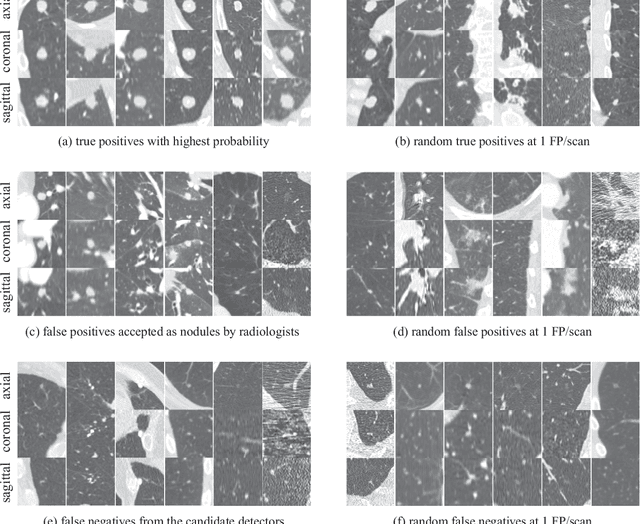
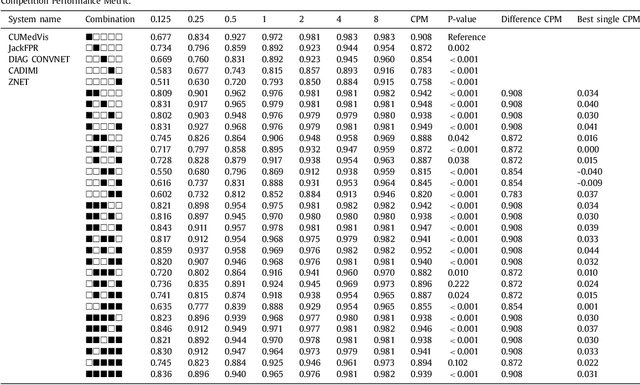
Automatic detection of pulmonary nodules in thoracic computed tomography (CT) scans has been an active area of research for the last two decades. However, there have only been few studies that provide a comparative performance evaluation of different systems on a common database. We have therefore set up the LUNA16 challenge, an objective evaluation framework for automatic nodule detection algorithms using the largest publicly available reference database of chest CT scans, the LIDC-IDRI data set. In LUNA16, participants develop their algorithm and upload their predictions on 888 CT scans in one of the two tracks: 1) the complete nodule detection track where a complete CAD system should be developed, or 2) the false positive reduction track where a provided set of nodule candidates should be classified. This paper describes the setup of LUNA16 and presents the results of the challenge so far. Moreover, the impact of combining individual systems on the detection performance was also investigated. It was observed that the leading solutions employed convolutional networks and used the provided set of nodule candidates. The combination of these solutions achieved an excellent sensitivity of over 95% at fewer than 1.0 false positives per scan. This highlights the potential of combining algorithms to improve the detection performance. Our observer study with four expert readers has shown that the best system detects nodules that were missed by expert readers who originally annotated the LIDC-IDRI data. We released this set of additional nodules for further development of CAD systems.