 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeHarmonization mitigates diffusion MRI scanner effects in infancy: insights from the HEALthy Brain and Childhood Development (HBCD) study
Mar 31, 2026The HEALthy Brain and Childhood Development (HBCD) Study is an ongoing longitudinal initiative to understand population-level brain maturation; however, large-scale studies must overcome site-related variance and preserve biologically relevant signal. In addition to diffusion-weighted magnetic resonance imaging images, the HBCD dataset offers analysis-ready derivatives for scientists to conduct their analysis, including scalar diffusion tensor (DTI) metrics in a predetermined set of bundles. The purpose of this study is to characterize HBCD-specific site effects in diffusion MRI data, which have not been systematically reported. In this work, we investigate the sensitivity of HBCD bundle metrics to scanner model-related variance and address these variations with ComBat-GAM harmonization within the current HBCD data release 1.1 across six scanner models. Following ComBat-GAM, we observe zero statistically significant differences between the distributions from any scanner model following FDR correction and reduce Cohen's f effect sizes across all metrics. Our work underscores the importance of rigorous harmonization efforts in large-scale studies, and we encourage future investigations of HBCD data to control for these effects.
Design Stability in Adaptive Experiments: Implications for Treatment Effect Estimation
Oct 25, 2025We study the problem of estimating the average treatment effect (ATE) under sequentially adaptive treatment assignment mechanisms. In contrast to classical completely randomized designs, we consider a setting in which the probability of assigning treatment to each experimental unit may depend on prior assignments and observed outcomes. Within the potential outcomes framework, we propose and analyze two natural estimators for the ATE: the inverse propensity weighted (IPW) estimator and an augmented IPW (AIPW) estimator. The cornerstone of our analysis is the concept of design stability, which requires that as the number of units grows, either the assignment probabilities converge, or sample averages of the inverse propensity scores and of the inverse complement propensity scores converge in probability to fixed, non-random limits. Our main results establish central limit theorems for both the IPW and AIPW estimators under design stability and provide explicit expressions for their asymptotic variances. We further propose estimators for these variances, enabling the construction of asymptotically valid confidence intervals. Finally, we illustrate our theoretical results in the context of Wei's adaptive coin design and Efron's biased coin design, highlighting the applicability of the proposed methods to sequential experimentation with adaptive randomization.
Body-mounted MR-conditional Robot for Minimally Invasive Liver Intervention
Oct 11, 2023MR-guided microwave ablation (MWA) has proven effective in treating hepatocellular carcinoma (HCC) with small-sized tumors, but the state-of-the-art technique suffers from sub-optimal workflow due to speed and accuracy of needle placement. This paper presents a compact body-mounted MR-conditional robot that can operate in closed-bore MR scanners for accurate needle guidance. The robotic platform consists of two stacked Cartesian XY stages, each with two degrees of freedom, that facilitate needle guidance. The robot is actuated using 3D-printed pneumatic turbines with MR-conditional bevel gear transmission systems. Pneumatic valves and control mechatronics are located inside the MRI control room and are connected to the robot with pneumatic transmission lines and optical fibers. Free space experiments indicated robot-assisted needle insertion error of 2.6$\pm$1.3 mm at an insertion depth of 80 mm. The MR-guided phantom studies were conducted to verify the MR-conditionality and targeting performance of the robot. Future work will focus on the system optimization and validations in animal trials.
A Surgical Platform for Intracerebral Hemorrhage Robotic Evacuation (ASPIHRE): A Non-metallic MR-guided Concentric Tube Robot
Jun 20, 2022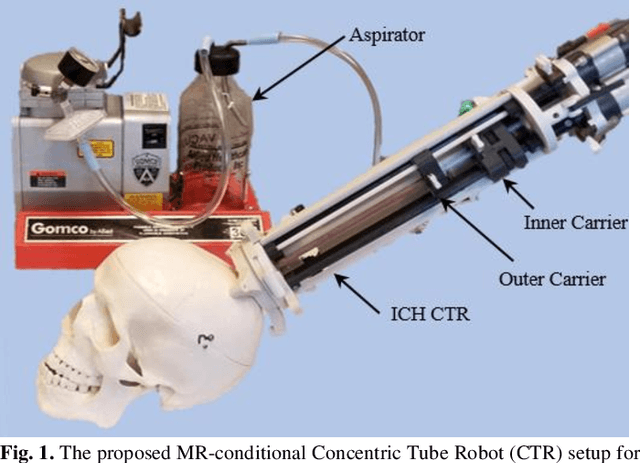
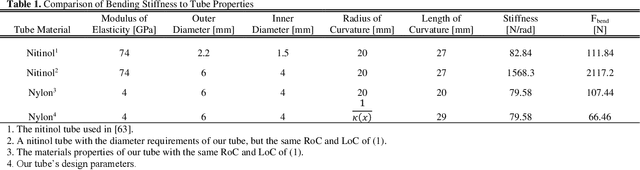
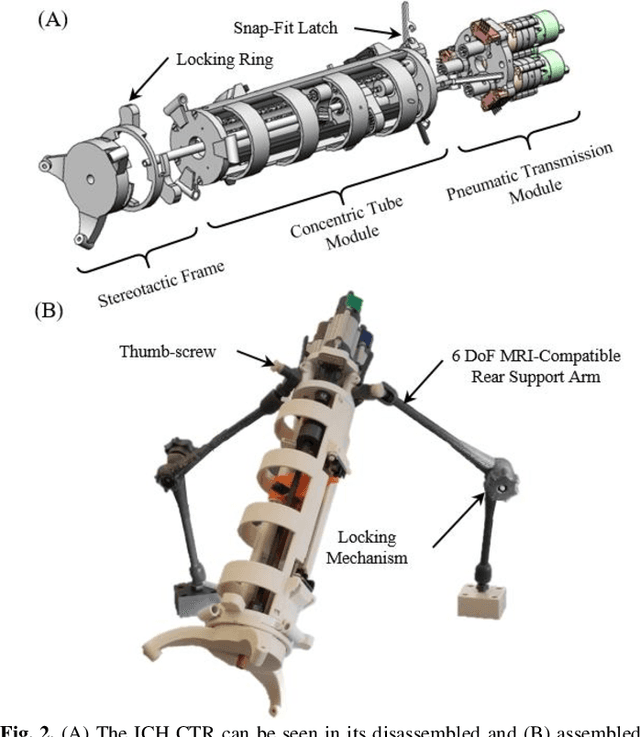
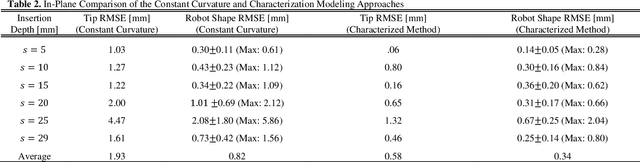
Intracerebral hemorrhage (ICH) is the deadliest stroke sub-type, with a one-month mortality rate as high as 52%. Due to the potential cortical disruption caused by craniotomy, conservative management (watchful waiting) has historically been a common method of treatment. Minimally invasive evacuation has recently become an accepted method of treatment for patients with deep-seated hematoma 30-50 mL in volume, but proper visualization and tool dexterity remain constrained in conventional endoscopic approaches, particularly with larger hematoma volumes (> 50 mL). In this article we describe the development of ASPIHRE (A Surgical Platform for Intracerebral Hemorrhage Robotic Evacuation), the first-ever concentric tube robot that uses off-the-shelf plastic tubes for MR-guided ICH evacuation, improving tool dexterity and procedural visualization. The robot kinematics model is developed based on a calibration-based method and tube mechanics modeling, allowing the models to consider both variable curvature and torsional deflection. The MR-safe pneumatic motors are controlled using a variable gain PID algorithm producing a rotational accuracy of 0.317 +/- 0.3 degrees. The hardware and theoretical models are validated in a series of systematic bench-top and MRI experiments resulting in positional accuracy of the tube tip of 1.39 +\- 0.54 mm. Following validation of targeting accuracy, the evacuation efficacy of the robot was tested in an MR-guided phantom clot evacuation experiment. The robot was able to evacuate an initially 38.36 mL clot in 5 minutes, leaving a residual hematoma of 8.14 mL, well below the 15 mL guideline suggesting good post-ICH evacuation clinical outcomes.