 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeVISTA Architect: A graph database-oriented health AI system demonstrated in multidisciplinary tumor boards
Jun 21, 2026We introduce VISTA Architect, a database-oriented AI architecture for integrating large language models (LLMs) with longitudinal electronic health records (EHRs). At ingestion, it transforms complex clinical documentation into a persistent, provenance-linked knowledge graph, eliminating repeated reprocessing of raw records at query time. The architecture has two layers: a source-faithful MEDS Graph preserving granular EHR structure with full provenance, and a clinically abstracted Timeline Object Architecture (TOA) that uses graph-guided LLM extraction to synthesize a concise timeline of deduplicated, temporally coherent clinical events. This addresses key limitations of direct long-context prompting and retrieval-augmented generation (RAG), which often miss temporal relationships and incur high cost and latency from repeated raw-text processing. By precomputing clinical synthesis once, downstream queries access an organized patient state and traverse to source documentation only when detailed verification is needed. We demonstrate the system in multidisciplinary thoracic oncology tumor boards at Stanford Medicine, where precise reconstruction of patient histories is critical. Across 1,180 patients, VISTA Architect achieved 96.4% accuracy (mean 9.75/10) on 15 tumor board-salient variables (17,700 evaluations; 95% CI 96.1-96.7%), surpassing a matched BM25 RAG baseline and recent benchmarks for LLM-based clinical extraction. An agentic interface reduced preparation for a 30-patient held-out cohort to about 2.2 minutes without sacrificing accuracy. While configured here for thoracic oncology, the modular design adapts to other specialties through customizable event definitions, episode structures, and agentic tools; validation beyond thoracic oncology remains future work.
Cooperative learning for multi-view analysis
Jan 06, 2022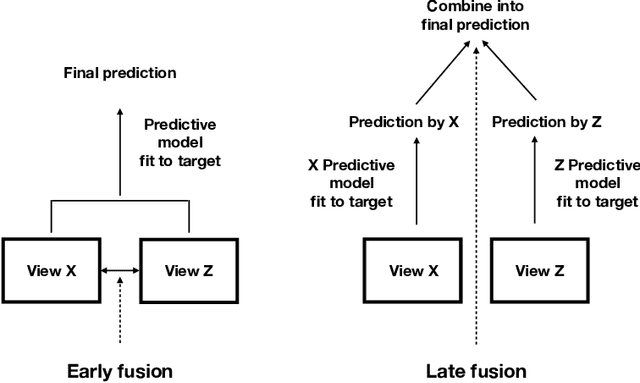
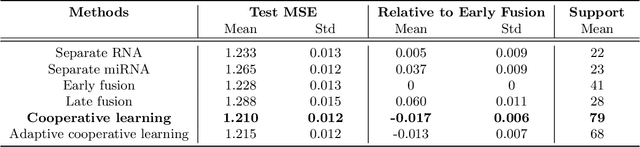
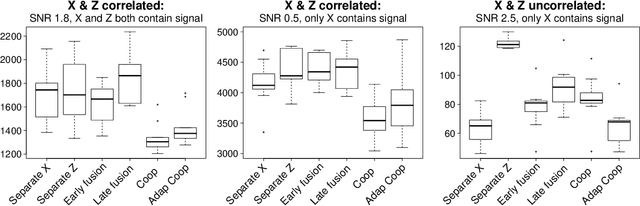
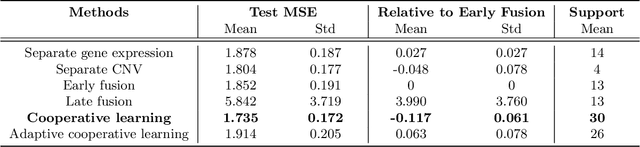
We propose a new method for supervised learning with multiple sets of features ("views"). Cooperative learning combines the usual squared error loss of predictions with an "agreement" penalty to encourage the predictions from different data views to agree. By varying the weight of the agreement penalty, we get a continuum of solutions that include the well-known early and late fusion approaches. Cooperative learning chooses the degree of agreement (or fusion) in an adaptive manner, using a validation set or cross-validation to estimate test set prediction error. One version of our fitting procedure is modular, where one can choose different fitting mechanisms (e.g. lasso, random forests, boosting, neural networks) appropriate for different data views. In the setting of cooperative regularized linear regression, the method combines the lasso penalty with the agreement penalty. The method can be especially powerful when the different data views share some underlying relationship in their signals that we aim to strengthen, while each view has its idiosyncratic noise that we aim to reduce. We illustrate the effectiveness of our proposed method on simulated and real data examples.
A Simple Discrete-Time Survival Model for Neural Networks
May 03, 2018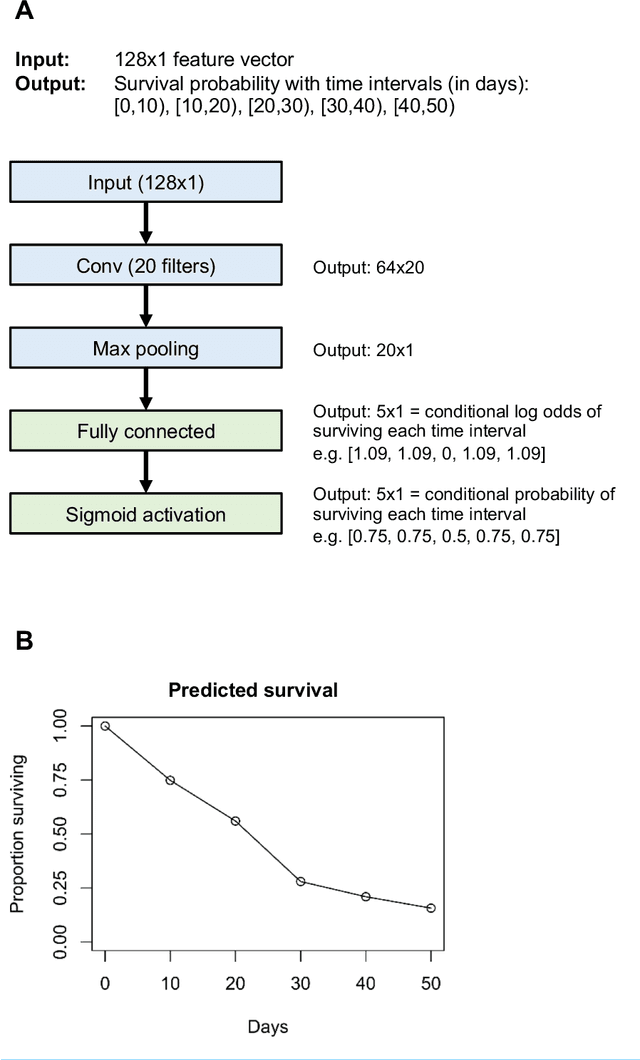
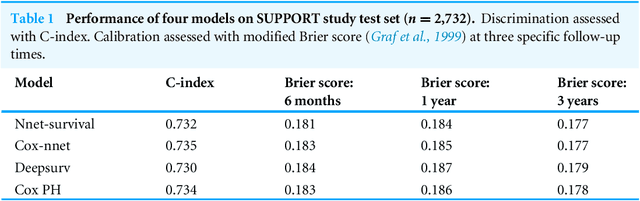
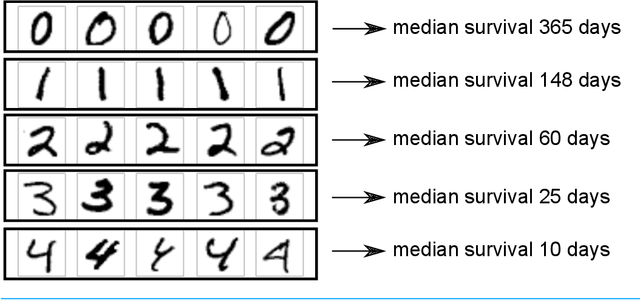
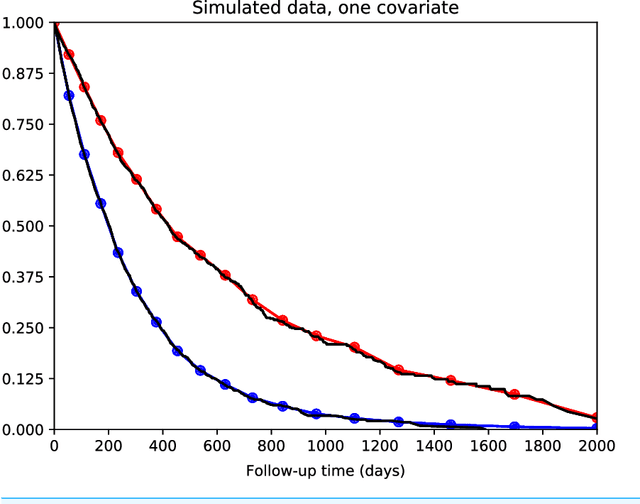
There is currently great interest in applying neural networks to prediction tasks in medicine. It is important for predictive models to be able to use survival data, where each patient has a known follow-up time and event/censoring indicator. This avoids information loss when training the model and enables generation of predicted survival curves. In this paper, we describe a discrete-time survival model that is designed to be used with neural networks. The model is trained with the maximum likelihood method using minibatch stochastic gradient descent (SGD). The use of SGD enables rapid training speed. The model is flexible, so that the baseline hazard rate and the effect of the input data can vary with follow-up time. It has been implemented in the Keras deep learning framework, and source code for the model and several examples is available online. We demonstrated the high performance of the model by using it as part of a convolutional neural network to predict survival for over 10,000 patients with metastatic cancer, using the full text of 1,137,317 provider notes. The model's C-index on the validation set was 0.71, which was superior to a linear baseline model (C-index 0.69).