 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeBone Suppression on Chest Radiographs With Adversarial Learning
Feb 08, 2020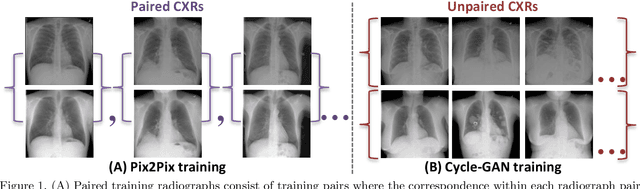
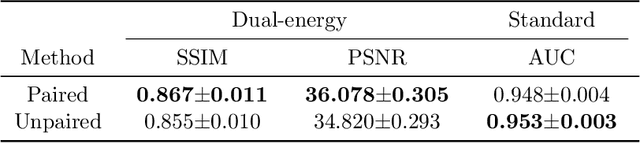
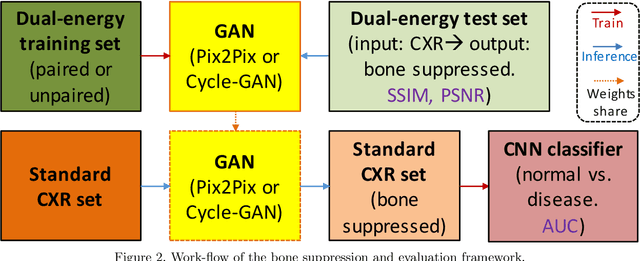
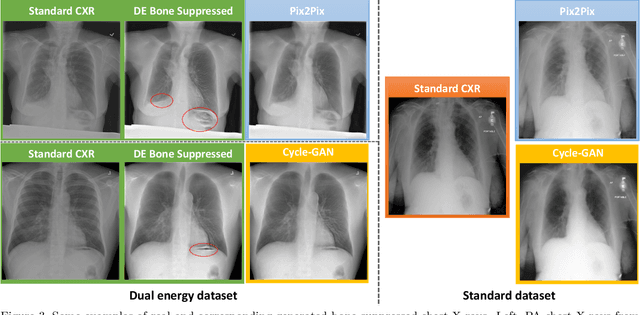
Dual-energy (DE) chest radiography provides the capability of selectively imaging two clinically relevant materials, namely soft tissues, and osseous structures, to better characterize a wide variety of thoracic pathology and potentially improve diagnosis in posteroanterior (PA) chest radiographs. However, DE imaging requires specialized hardware and a higher radiation dose than conventional radiography, and motion artifacts sometimes happen due to involuntary patient motion. In this work, we learn the mapping between conventional radiographs and bone suppressed radiographs. Specifically, we propose to utilize two variations of generative adversarial networks (GANs) for image-to-image translation between conventional and bone suppressed radiographs obtained by DE imaging technique. We compare the effectiveness of training with patient-wisely paired and unpaired radiographs. Experiments show both training strategies yield "radio-realistic'' radiographs with suppressed bony structures and few motion artifacts on a hold-out test set. While training with paired images yields slightly better performance than that of unpaired images when measuring with two objective image quality metrics, namely Structural Similarity Index (SSIM) and Peak Signal-to-Noise Ratio (PSNR), training with unpaired images demonstrates better generalization ability on unseen anteroposterior (AP) radiographs than paired training.
Accurately identifying vertebral levels in large datasets
Jan 28, 2020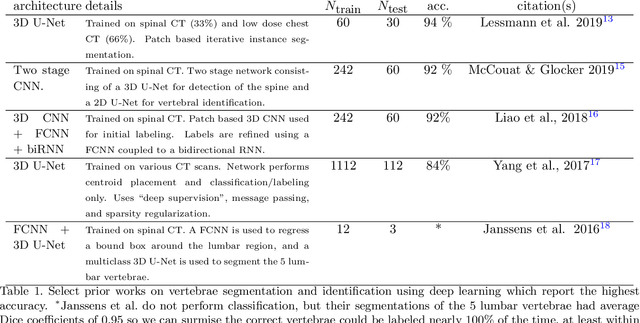
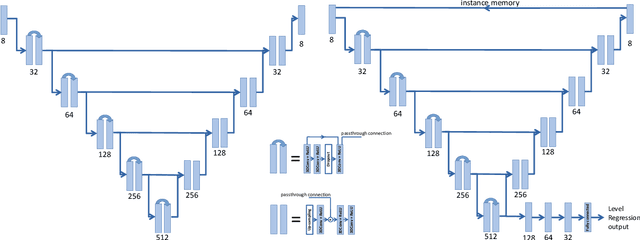
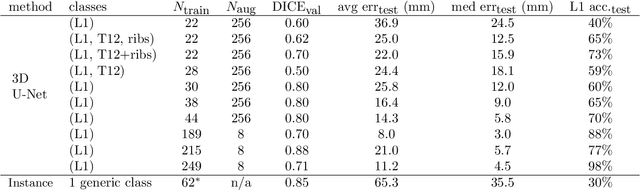

The vertebral levels of the spine provide a useful coordinate system when making measurements of plaque, muscle, fat, and bone mineral density. Correctly classifying vertebral levels with high accuracy is challenging due to the similar appearance of each vertebra, the curvature of the spine, and the possibility of anomalies such as fractured vertebrae, implants, lumbarization of the sacrum, and sacralization of L5. The goal of this work is to develop a system that can accurately and robustly identify the L1 level in large heterogeneous datasets. The first approach we study is using a 3D U-Net to segment the L1 vertebra directly using the entire scan volume to provide context. We also tested models for two class segmentation of L1 and T12 and a three class segmentation of L1, T12 and the rib attached to T12. By increasing the number of training examples to 249 scans using pseudo-segmentations from an in-house segmentation tool we were able to achieve 98% accuracy with respect to identifying the L1 vertebra, with an average error of 4.5 mm in the craniocaudal level. We next developed an algorithm which performs iterative instance segmentation and classification of the entire spine with a 3D U-Net. We found the instance based approach was able to yield better segmentations of nearly the entire spine, but had lower classification accuracy for L1.
Weakly Supervised Lesion Co-segmentation on CT Scans
Jan 24, 2020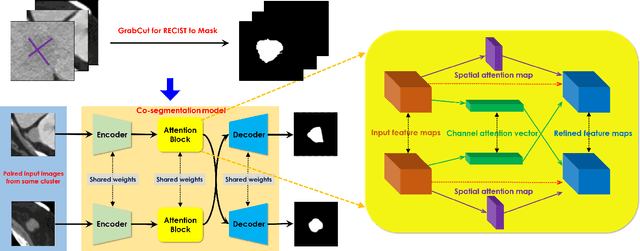


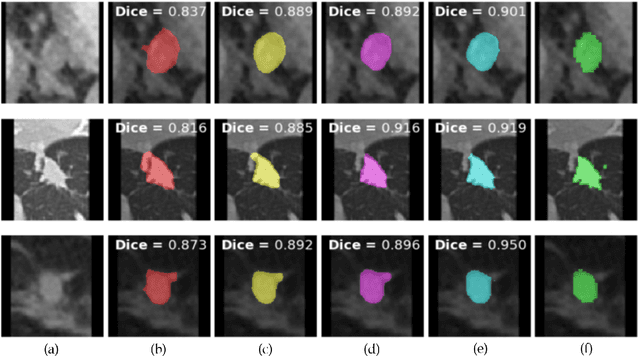
Lesion segmentation in medical imaging serves as an effective tool for assessing tumor sizes and monitoring changes in growth. However, not only is manual lesion segmentation time-consuming, but it is also expensive and requires expert radiologist knowledge. Therefore many hospitals rely on a loose substitute called response evaluation criteria in solid tumors (RECIST). Although these annotations are far from precise, they are widely used throughout hospitals and are found in their picture archiving and communication systems (PACS). Therefore, these annotations have the potential to serve as a robust yet challenging means of weak supervision for training full lesion segmentation models. In this work, we propose a weakly-supervised co-segmentation model that first generates pseudo-masks from the RECIST slices and uses these as training labels for an attention-based convolutional neural network capable of segmenting common lesions from a pair of CT scans. To validate and test the model, we utilize the DeepLesion dataset, an extensive CT-scan lesion dataset that contains 32,735 PACS bookmarked images. Extensive experimental results demonstrate the efficacy of our co-segmentation approach for lesion segmentation with a mean Dice coefficient of 90.3%.
Weakly-Supervised Lesion Segmentation on CT Scans using Co-Segmentation
Jan 23, 2020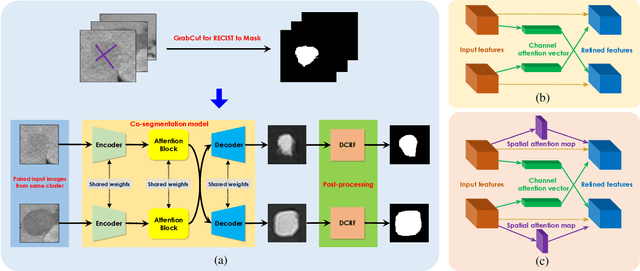
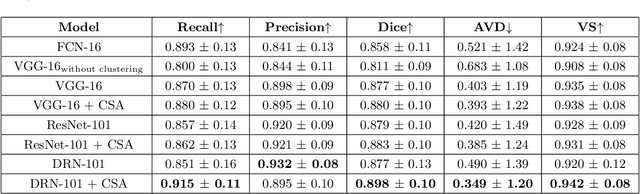
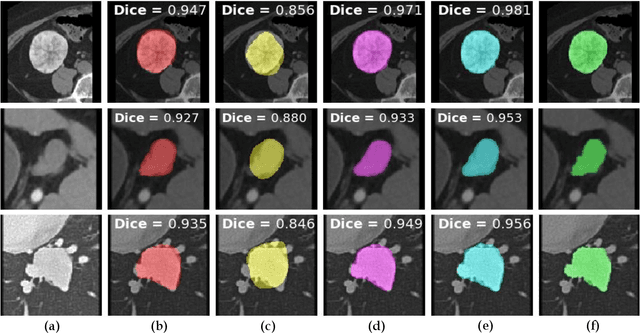
Lesion segmentation on computed tomography (CT) scans is an important step for precisely monitoring changes in lesion/tumor growth. This task, however, is very challenging since manual segmentation is prohibitively time-consuming, expensive, and requires professional knowledge. Current practices rely on an imprecise substitute called response evaluation criteria in solid tumors (RECIST). Although these markers lack detailed information about the lesion regions, they are commonly found in hospitals' picture archiving and communication systems (PACS). Thus, these markers have the potential to serve as a powerful source of weak-supervision for 2D lesion segmentation. To approach this problem, this paper proposes a convolutional neural network (CNN) based weakly-supervised lesion segmentation method, which first generates the initial lesion masks from the RECIST measurements and then utilizes co-segmentation to leverage lesion similarities and refine the initial masks. In this work, an attention-based co-segmentation model is adopted due to its ability to learn more discriminative features from a pair of images. Experimental results on the NIH DeepLesion dataset demonstrate that the proposed co-segmentation approach significantly improves lesion segmentation performance, e.g the Dice score increases about 4.0% (from 85.8% to 89.8%).
$Σ$-net: Systematic Evaluation of Iterative Deep Neural Networks for Fast Parallel MR Image Reconstruction
Dec 18, 2019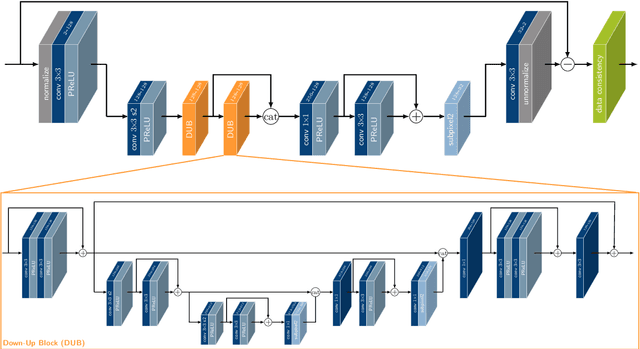
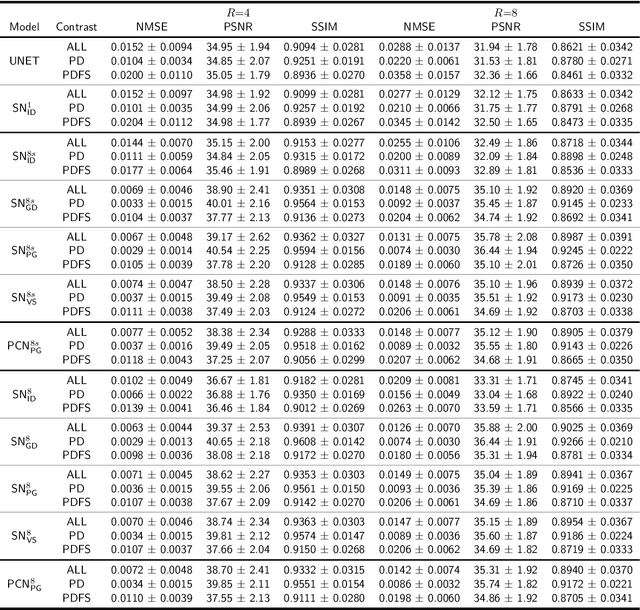
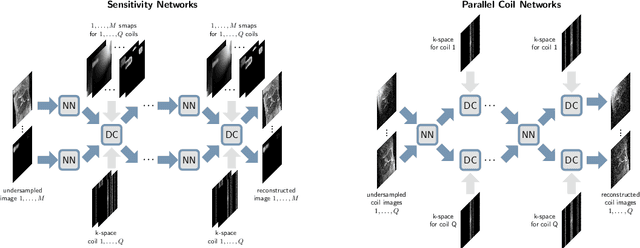
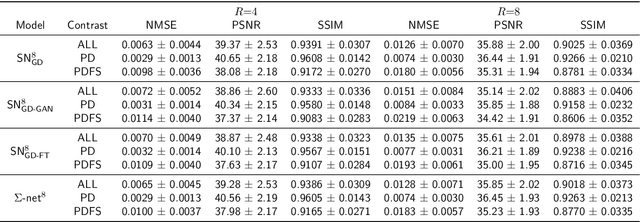
Purpose: To systematically investigate the influence of various data consistency layers, (semi-)supervised learning and ensembling strategies, defined in a $\Sigma$-net, for accelerated parallel MR image reconstruction using deep learning. Theory and Methods: MR image reconstruction is formulated as learned unrolled optimization scheme with a Down-Up network as regularization and varying data consistency layers. The different architectures are split into sensitivity networks, which rely on explicit coil sensitivity maps, and parallel coil networks, which learn the combination of coils implicitly. Different content and adversarial losses, a semi-supervised fine-tuning scheme and model ensembling are investigated. Results: Evaluated on the fastMRI multicoil validation set, architectures involving raw k-space data outperform image enhancement methods significantly. Semi-supervised fine-tuning adapts to new k-space data and provides, together with reconstructions based on adversarial training, the visually most appealing results although quantitative quality metrics are reduced. The $\Sigma$-net ensembles the benefits from different models and achieves similar scores compared to the single state-of-the-art approaches. Conclusion: This work provides an open-source framework to perform a systematic wide-range comparison of state-of-the-art reconstruction approaches for parallel MR image reconstruction on the fastMRI knee dataset and explores the importance of data consistency. A suitable trade-off between perceptual image quality and quantitative scores are achieved with the ensembled $\Sigma$-net.
$Σ$-net: Ensembled Iterative Deep Neural Networks for Accelerated Parallel MR Image Reconstruction
Dec 11, 2019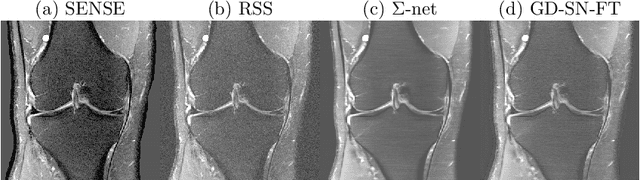
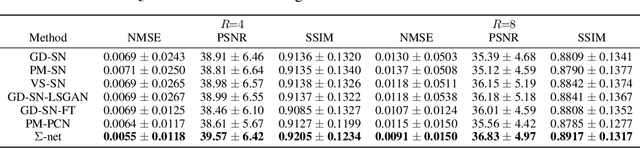
We explore an ensembled $\Sigma$-net for fast parallel MR imaging, including parallel coil networks, which perform implicit coil weighting, and sensitivity networks, involving explicit sensitivity maps. The networks in $\Sigma$-net are trained in a supervised way, including content and GAN losses, and with various ways of data consistency, i.e., proximal mappings, gradient descent and variable splitting. A semi-supervised finetuning scheme allows us to adapt to the k-space data at test time, which, however, decreases the quantitative metrics, although generating the visually most textured and sharp images. For this challenge, we focused on robust and high SSIM scores, which we achieved by ensembling all models to a $\Sigma$-net.
TUNA-Net: Task-oriented UNsupervised Adversarial Network for Disease Recognition in Cross-Domain Chest X-rays
Aug 21, 2019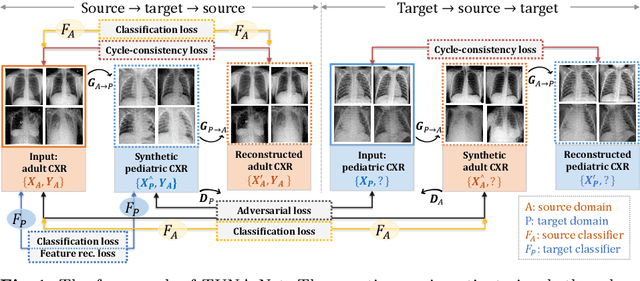
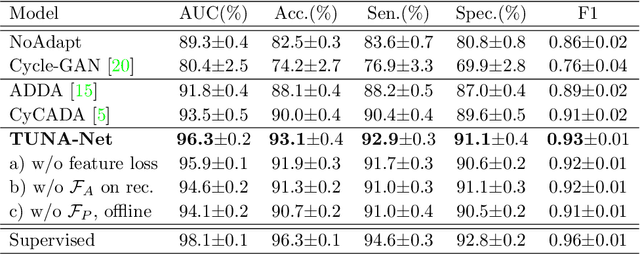
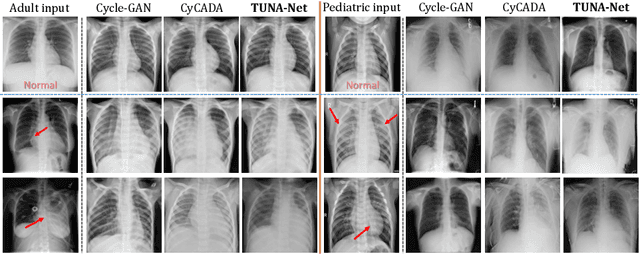
In this work, we exploit the unsupervised domain adaptation problem for radiology image interpretation across domains. Specifically, we study how to adapt the disease recognition model from a labeled source domain to an unlabeled target domain, so as to reduce the effort of labeling each new dataset. To address the shortcoming of cross-domain, unpaired image-to-image translation methods which typically ignore class-specific semantics, we propose a task-driven, discriminatively trained, cycle-consistent generative adversarial network, termed TUNA-Net. It is able to preserve 1) low-level details, 2) high-level semantic information and 3) mid-level feature representation during the image-to-image translation process, to favor the target disease recognition task. The TUNA-Net framework is general and can be readily adapted to other learning tasks. We evaluate the proposed framework on two public chest X-ray datasets for pneumonia recognition. The TUNA-Net model can adapt labeled adult chest X-rays in the source domain such that they appear as if they were drawn from pediatric X-rays in the unlabeled target domain, while preserving the disease semantics. Extensive experiments show the superiority of the proposed method as compared to state-of-the-art unsupervised domain adaptation approaches. Notably, TUNA-Net achieves an AUC of 96.3% for pediatric pneumonia classification, which is very close to that of the supervised approach (98.1%), but without the need for labels on the target domain.
MULAN: Multitask Universal Lesion Analysis Network for Joint Lesion Detection, Tagging, and Segmentation
Aug 12, 2019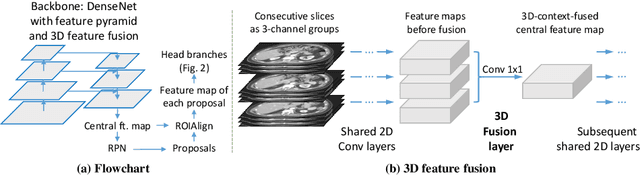
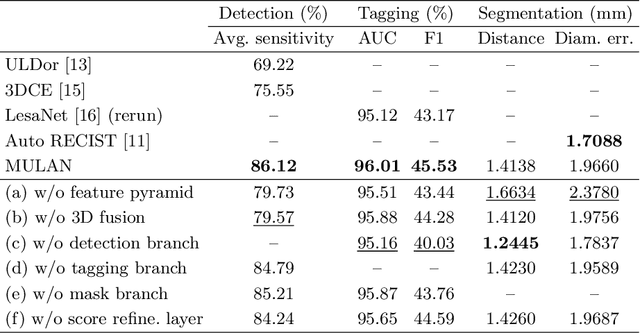
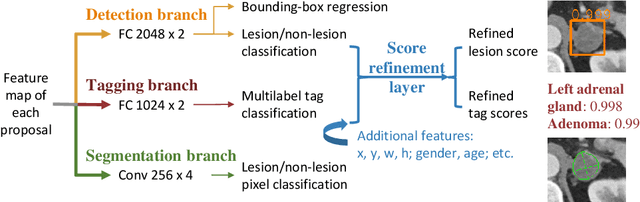
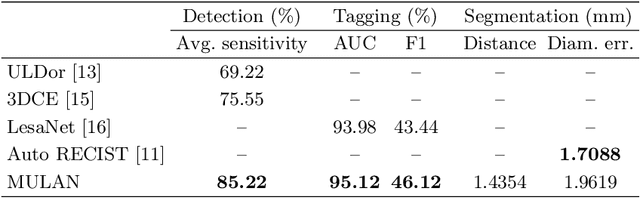
When reading medical images such as a computed tomography (CT) scan, radiologists generally search across the image to find lesions, characterize and measure them, and then describe them in the radiological report. To automate this process, we propose a multitask universal lesion analysis network (MULAN) for joint detection, tagging, and segmentation of lesions in a variety of body parts, which greatly extends existing work of single-task lesion analysis on specific body parts. MULAN is based on an improved Mask R-CNN framework with three head branches and a 3D feature fusion strategy. It achieves the state-of-the-art accuracy in the detection and tagging tasks on the DeepLesion dataset, which contains 32K lesions in the whole body. We also analyze the relationship between the three tasks and show that tag predictions can improve detection accuracy via a score refinement layer.
A self-attention based deep learning method for lesion attribute detection from CT reports
Apr 30, 2019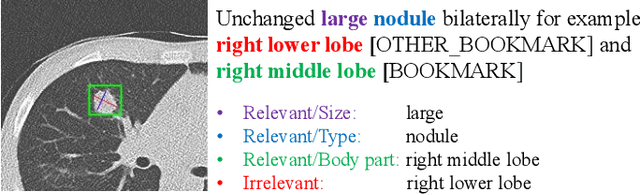
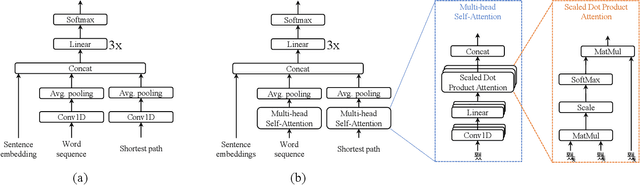
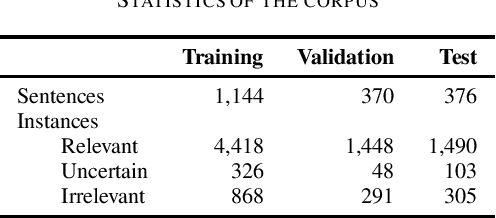
In radiology, radiologists not only detect lesions from the medical image, but also describe them with various attributes such as their type, location, size, shape, and intensity. While these lesion attributes are rich and useful in many downstream clinical applications, how to extract them from the radiology reports is less studied. This paper outlines a novel deep learning method to automatically extract attributes of lesions of interest from the clinical text. Different from classical CNN models, we integrated the multi-head self-attention mechanism to handle the long-distance information in the sentence, and to jointly correlate different portions of sentence representation subspaces in parallel. Evaluation on an in-house corpus demonstrates that our method can achieve high performance with 0.848 in precision, 0.788 in recall, and 0.815 in F-score. The new method and constructed corpus will enable us to build automatic systems with a higher-level understanding of the radiological world.
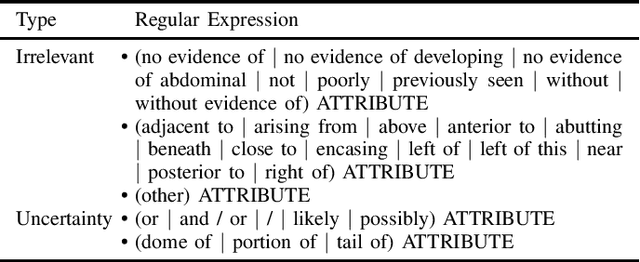
Holistic and Comprehensive Annotation of Clinically Significant Findings on Diverse CT Images: Learning from Radiology Reports and Label Ontology
Apr 27, 2019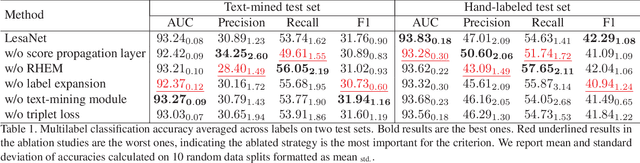
In radiologists' routine work, one major task is to read a medical image, e.g., a CT scan, find significant lesions, and describe them in the radiology report. In this paper, we study the lesion description or annotation problem. Given a lesion image, our aim is to predict a comprehensive set of relevant labels, such as the lesion's body part, type, and attributes, which may assist downstream fine-grained diagnosis. To address this task, we first design a deep learning module to extract relevant semantic labels from the radiology reports associated with the lesion images. With the images and text-mined labels, we propose a lesion annotation network (LesaNet) based on a multilabel convolutional neural network (CNN) to learn all labels holistically. Hierarchical relations and mutually exclusive relations between the labels are leveraged to improve the label prediction accuracy. The relations are utilized in a label expansion strategy and a relational hard example mining algorithm. We also attach a simple score propagation layer on LesaNet to enhance recall and explore implicit relation between labels. Multilabel metric learning is combined with classification to enable interpretable prediction. We evaluated LesaNet on the public DeepLesion dataset, which contains over 32K diverse lesion images. Experiments show that LesaNet can precisely annotate the lesions using an ontology of 171 fine-grained labels with an average AUC of 0.9344.