 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeContour-Constrained Deformable Registration with Parameter Characterization for Head and Neck Surgical Guidance
Jun 18, 2026With 890,000 annual new cases globally, head and neck squamous cell carcinoma has one of the highest recurrence rates among solid malignancies. Although frozen section analysis is the standard of care for intraoperative margin assessment, accurately relocating detected positive margins on the resection bed remains challenging due to imprecise alignment between resected specimens and their resection bed, compounded by post-resection mucosal tissue shrinkage. We present a biomechanics-driven deformable registration framework that corrects post-resection tissue deformation to provide intraoperative guidance. Our approach registers 3D specimen meshes to intraoperative resection bed point clouds using a deformable registration approach based on regularized Kelvinlet basis functions. The registration matches surface point clouds, fiducial landmarks, and boundary contour constraints that directly penalize perpendicular distance-to-agreement between specimen and resection bed boundaries. Across nine specimens from skin, buccal mucosa, and tongue sites, the overall mean target registration error was $11.11 \pm 4.07$ mm using rigid registration, which decreased to $8.20 \pm 2.68$ mm (26.19\% reduction) using deformable registration without contour constraint. The proposed contour-constrained deformable registration further reduced the error to $5.62 \pm 2.28$ mm, a 49.41\% reduction relative to rigid registration. We observed the largest reduction in the most clinically challenging tongue specimens. We also performed a systematic two-stage parameter search to characterize the relative importance of surface alignment, fiducial correspondences, contour constraint, and strain energy regularization. This search revealed that contour weighting dominates registration accuracy for tissue types with large lateral deformation, while the algorithm operates over a broad range of parameter combinations.
All-in-One Augmented Reality Guided Head and Neck Tumor Resection
Mar 31, 2026Positive margins are common in head and neck squamous cell carcinoma, yet intraoperative re-resection is often imprecise because margin locations are typically communicated verbally from pathology. We present an all-in-one augmented reality (AR) system that relocalizes positive margins from a resected specimen to the resection bed and visualizes them in situ using HoloLens 2 depth sensing and fully automated markerless surface registration. In a silicone phantom study with six medical trainees, markerless registration achieved target registration errors comparable to a marker-based baseline (median 1.8 mm vs. 1.7 mm; maximum < 4 mm). In a margin relocalization task, AR guidance reduced error from verbal guidance (median 14.2 mm) to a few millimeters (median 3.2 mm), with all AR localizations within 5 mm error. These results support the feasibility of markerless AR margin guidance for more precise intraoperative re-excision.
Automated Assessment of Kidney Ureteroscopy Exploration for Training
Feb 17, 2026Purpose: Kidney ureteroscopic navigation is challenging with a steep learning curve. However, current clinical training has major deficiencies, as it requires one-on-one feedback from experts and occurs in the operating room (OR). Therefore, there is a need for a phantom training system with automated feedback to greatly \revision{expand} training opportunities. Methods: We propose a novel, purely ureteroscope video-based scope localization framework that automatically identifies calyces missed by the trainee in a phantom kidney exploration. We use a slow, thorough, prior exploration video of the kidney to generate a reference reconstruction. Then, this reference reconstruction can be used to localize any exploration video of the same phantom. Results: In 15 exploration videos, a total of 69 out of 74 calyces were correctly classified. We achieve < 4mm camera pose localization error. Given the reference reconstruction, the system takes 10 minutes to generate the results for a typical exploration (1-2 minute long). Conclusion: We demonstrate a novel camera localization framework that can provide accurate and automatic feedback for kidney phantom explorations. We show its ability as a valid tool that enables out-of-OR training without requiring supervision from an expert.
RESECT-SEG: Open access annotations of intra-operative brain tumor ultrasound images
Jul 13, 2022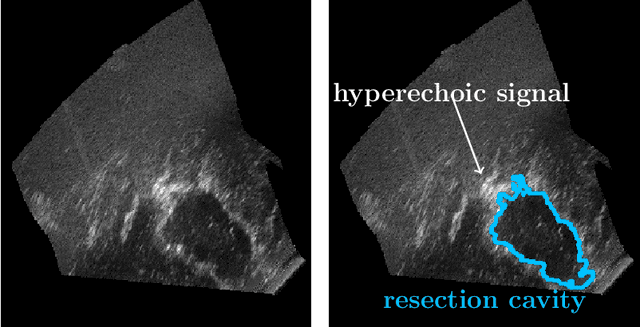
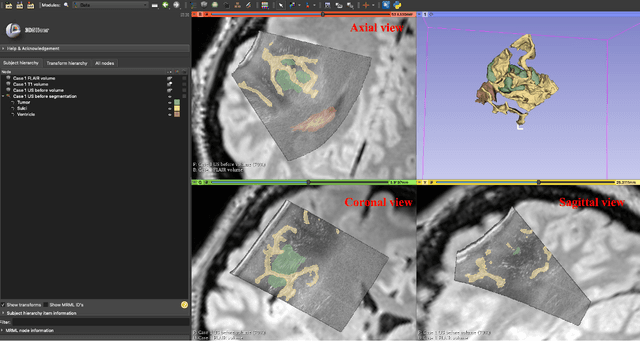
Purpose: Registration and segmentation of magnetic resonance (MR) and ultrasound (US) images play an essential role in surgical planning and resection of brain tumors. However, validating these techniques is challenging due to the scarcity of publicly accessible sources with high-quality ground truth information. To this end, we propose a unique annotation dataset of tumor tissues and resection cavities from the previously published RESECT dataset (Xiao et al. 2017) to encourage a more rigorous assessments of image processing techniques. Acquisition and validation methods: The RESECT database consists of MR and intraoperative US (iUS) images of 23 patients who underwent resection surgeries. The proposed dataset contains tumor tissues and resection cavity annotations of the iUS images. The quality of annotations were validated by two highly experienced neurosurgeons through several assessment criteria. Data format and availability: Annotations of tumor tissues and resection cavities are provided in 3D NIFTI formats. Both sets of annotations are accessible online in the \url{https://osf.io/6y4db}. Discussion and potential applications: The proposed database includes tumor tissue and resection cavity annotations from real-world clinical ultrasound brain images to evaluate segmentation and registration methods. These labels could also be used to train deep learning approaches. Eventually, this dataset should further improve the quality of image guidance in neurosurgery.