 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMARCUS: An agentic, multimodal vision-language model for cardiac diagnosis and management
Mar 23, 2026Cardiovascular disease remains the leading cause of global mortality, with progress hindered by human interpretation of complex cardiac tests. Current AI vision-language models are limited to single-modality inputs and are non-interactive. We present MARCUS (Multimodal Autonomous Reasoning and Chat for Ultrasound and Signals), an agentic vision-language system for end-to-end interpretation of electrocardiograms (ECGs), echocardiograms, and cardiac magnetic resonance imaging (CMR) independently and as multimodal input. MARCUS employs a hierarchical agentic architecture comprising modality-specific vision-language expert models, each integrating domain-trained visual encoders with multi-stage language model optimization, coordinated by a multimodal orchestrator. Trained on 13.5 million images (0.25M ECGs, 1.3M echocardiogram images, 12M CMR images) and our novel expert-curated dataset spanning 1.6 million questions, MARCUS achieves state-of-the-art performance surpassing frontier models (GPT-5 Thinking, Gemini 2.5 Pro Deep Think). Across internal (Stanford) and external (UCSF) test cohorts, MARCUS achieves accuracies of 87-91% for ECG, 67-86% for echocardiography, and 85-88% for CMR, outperforming frontier models by 34-45% (P<0.001). On multimodal cases, MARCUS achieved 70% accuracy, nearly triple that of frontier models (22-28%), with 1.7-3.0x higher free-text quality scores. Our agentic architecture also confers resistance to mirage reasoning, whereby vision-language models derive reasoning from unintended textual signals or hallucinated visual content. MARCUS demonstrates that domain-specific visual encoders with an agentic orchestrator enable multimodal cardiac interpretation. We release our models, code, and benchmark open-source.
Predicting post-operative right ventricular failure using video-based deep learning
Feb 28, 2021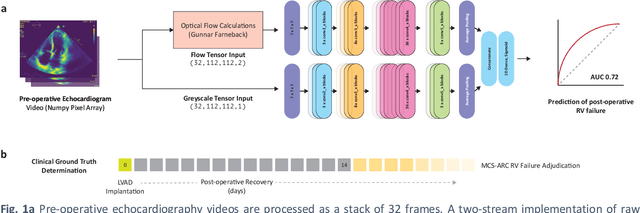
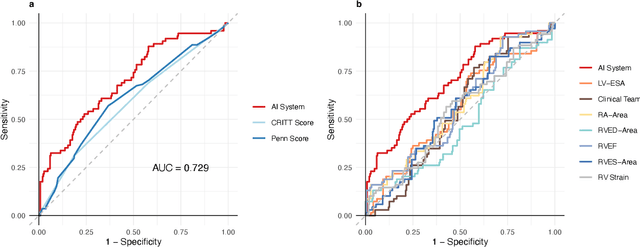
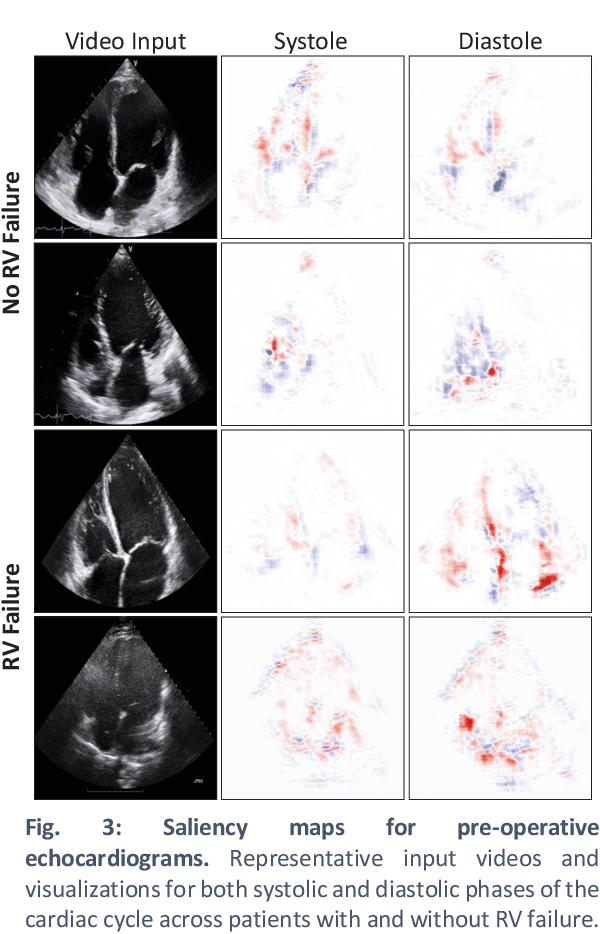
Non-invasive and cost effective in nature, the echocardiogram allows for a comprehensive assessment of the cardiac musculature and valves. Despite progressive improvements over the decades, the rich temporally resolved data in echocardiography videos remain underutilized. Human reads of echocardiograms reduce the complex patterns of cardiac wall motion, to a small list of measurements of heart function. Furthermore, all modern echocardiography artificial intelligence (AI) systems are similarly limited by design - automating measurements of the same reductionist metrics rather than utilizing the wealth of data embedded within each echo study. This underutilization is most evident in situations where clinical decision making is guided by subjective assessments of disease acuity, and tools that predict disease onset within clinically actionable timeframes are unavailable. Predicting the likelihood of developing post-operative right ventricular failure (RV failure) in the setting of mechanical circulatory support is one such clinical example. To address this, we developed a novel video AI system trained to predict post-operative right ventricular failure (RV failure), using the full spatiotemporal density of information from pre-operative echocardiography scans. We achieve an AUC of 0.729, specificity of 52% at 80% sensitivity and 46% sensitivity at 80% specificity. Furthermore, we show that our ML system significantly outperforms a team of human experts tasked with predicting RV failure on independent clinical evaluation. Finally, the methods we describe are generalizable to any cardiac clinical decision support application where treatment or patient selection is guided by qualitative echocardiography assessments.