 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeKhala: Scaling Acoustic Token Language Models Toward High-Fidelity Music Generation
May 03, 2026A common design pattern in high-quality music generation is to handle structure and fidelity in different representation spaces: a generator first models high-level structure, followed by diffusion-based or neural decoding stages that reconstruct fine details. In this work, we explore an alternative view: both may be progressively modeled within a single deep acoustic-token hierarchy. To study this, we build a 64-layer residual vector quantization (RVQ) acoustic representation and propose a two-stage coarse-to-fine generation framework. A backbone model first generates coarse acoustic tokens for the full track, and a super-resolution model then completes finer tokens within the same acoustic token space. The super-resolution stage works at full-track scale and refines tokens layer by layer while running in parallel over time, leading to a fixed 62-step inference process. To jointly improve lyric alignment and fine-detail reconstruction, we further introduce hybrid-attention training: the alignment objective uses causal attention, while layer-wise refinement uses full attention. A key finding is that text--vocal alignment can emerge within pure acoustic-token language modeling, without requiring a separate semantic token stage. Moreover, initializing the super-resolution model from the trained backbone significantly improves convergence and final quality. Taken together, our results suggest that high-quality music generation can be effectively pursued without separating structure and fidelity into heterogeneous representation spaces. Instead, both can be progressively modeled within a unified acoustic-token hierarchy, pointing toward a simpler and more unified path to high-quality music generation.
IMUVIE: Pickup Timeline Action Localization via Motion Movies
Nov 19, 2024



Falls among seniors due to difficulties with tasks such as picking up objects pose significant health and safety risks, impacting quality of life and independence. Reliable, accessible assessment tools are critical for early intervention but often require costly clinic-based equipment and trained personnel, limiting their use in daily life. Existing wearable-based pickup measurement solutions address some needs but face limitations in generalizability. We present IMUVIE, a wearable system that uses motion movies and a machine-learning model to automatically detect and measure pickup events, providing a practical solution for frequent monitoring. IMUVIE's design principles-data normalization, occlusion handling, and streamlined visuals-enhance model performance and are adaptable to tasks beyond pickup classification. In rigorous leave one subject out cross validation evaluations, IMUVIE achieves exceptional window level localization accuracy of 91-92% for pickup action classification on 256,291 motion movie frame candidates while maintaining an event level recall of 97% when evaluated on 129 pickup events. IMUVIE has strong generalization and performs well on unseen subjects. In an interview survey, IMUVIE demonstrated strong user interest and trust, with ease of use identified as the most critical factor for adoption. IMUVIE offers a practical, at-home solution for fall risk assessment, facilitating early detection of movement deterioration, and supporting safer, independent living for seniors.
Penalized Deep Partially Linear Cox Models with Application to CT Scans of Lung Cancer Patients
Mar 09, 2023



Lung cancer is a leading cause of cancer mortality globally, highlighting the importance of understanding its mortality risks to design effective patient-centered therapies. The National Lung Screening Trial (NLST) was a nationwide study aimed at investigating risk factors for lung cancer. The study employed computed tomography texture analysis (CTTA), which provides objective measurements of texture patterns on CT scans, to quantify the mortality risks of lung cancer patients. Partially linear Cox models are becoming a popular tool for modeling survival outcomes, as they effectively handle both established risk factors (such as age and other clinical factors) and new risk factors (such as image features) in a single framework. The challenge in identifying the texture features that impact cancer survival is due to their sensitivity to factors such as scanner type, segmentation, and organ motion. To overcome this challenge, we propose a novel Penalized Deep Partially Linear Cox Model (Penalized DPLC), which incorporates the SCAD penalty to select significant texture features and employs a deep neural network to estimate the nonparametric component of the model accurately. We prove the convergence and asymptotic properties of the estimator and compare it to other methods through extensive simulation studies, evaluating its performance in risk prediction and feature selection. The proposed method is applied to the NLST study dataset to uncover the effects of key clinical and imaging risk factors on patients' survival. Our findings provide valuable insights into the relationship between these factors and survival outcomes.
Individualized Risk Assessment of Preoperative Opioid Use by Interpretable Neural Network Regression
May 07, 2022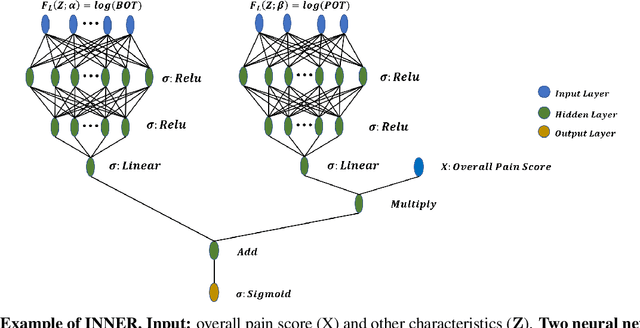
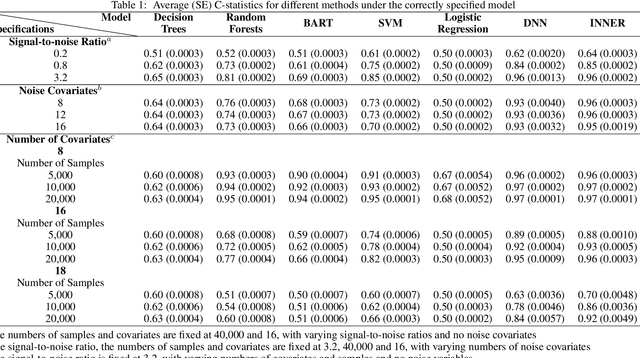
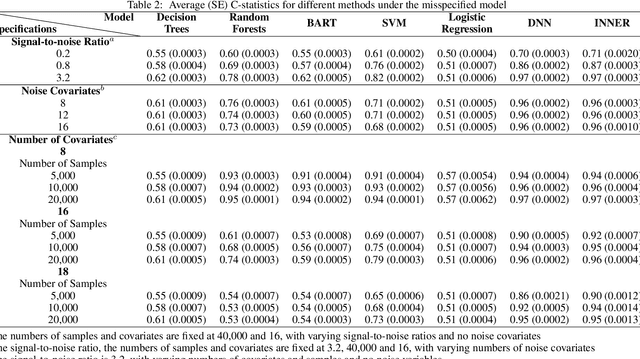
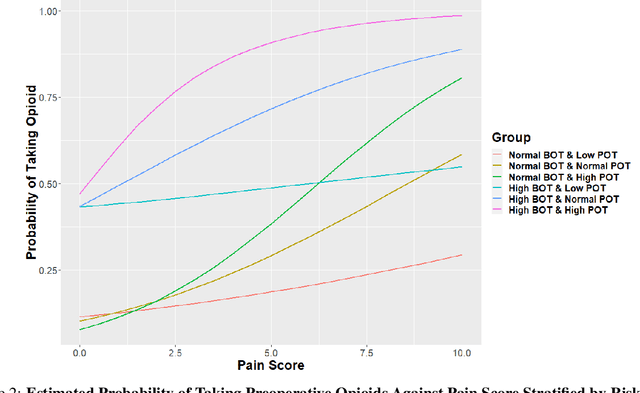
Preoperative opioid use has been reported to be associated with higher preoperative opioid demand, worse postoperative outcomes, and increased postoperative healthcare utilization and expenditures. Understanding the risk of preoperative opioid use helps establish patient-centered pain management. In the field of machine learning, deep neural network (DNN) has emerged as a powerful means for risk assessment because of its superb prediction power; however, the blackbox algorithms may make the results less interpretable than statistical models. Bridging the gap between the statistical and machine learning fields, we propose a novel Interpretable Neural Network Regression (INNER), which combines the strengths of statistical and DNN models. We use the proposed INNER to conduct individualized risk assessment of preoperative opioid use. Intensive simulations and an analysis of 34,186 patients expecting surgery in the Analgesic Outcomes Study (AOS) show that the proposed INNER not only can accurately predict the preoperative opioid use using preoperative characteristics as DNN, but also can estimate the patient specific odds of opioid use without pain and the odds ratio of opioid use for a unit increase in the reported overall body pain, leading to more straightforward interpretations of the tendency to use opioids than DNN. Our results identify the patient characteristics that are strongly associated with opioid use and is largely consistent with the previous findings, providing evidence that INNER is a useful tool for individualized risk assessment of preoperative opioid use.