 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeAssociation of Progressive PPFE and Mortality in Lung Cancer Screening Cohorts
Mar 17, 2026Background: Pleuroparenchymal fibroelastosis (PPFE) is an upper lobe predominant fibrotic lung abnormality associated with increased mortality in established interstitial lung disease. However, the clinical significance of radiologic PPFE progression in lung cancer screening (LCS) populations remains unclear. Methods: We analysed longitudinal low-dose CT scans and clinical data from two LCS studies: National Lung Screening Trial (NLST; n=7,980); SUMMIT study (n=8,561). An automated algorithm quantified PPFE volume on baseline and follow-up scans. Annualised change in PPFE was derived and dichotomised using a distribution-based threshold to define progressive PPFE. Associations between progressive PPFE and mortality were evaluated using Cox proportional hazards models adjusted for demographic and clinical variables. In SUMMIT cohort, associations between progressive PPFE and clinical outcomes were assessed using incidence rate ratios (IRR) and odds ratios (OR). Findings: Progressive PPFE independently associated with mortality in both LCS cohorts (NLST: Hazard Ratio (HR)=1.25, 95% Confidence Interval (CI): 1.01--1.56, p=0.042; SUMMIT: HR=3.14, 95% CI: 1.66--5.97, p<0.001). Within SUMMIT, progressive PPFE was strongly associated with higher respiratory admissions (IRR=2.79, p<0.001), increased antibiotic and steroid use (IRR=1.55, p=0.010), and showed a trend towards higher modified medical research council scores (OR=1.40, p=0.055). Interpretation: Radiologic PPFE progression independently associates with mortality across two large LCS cohorts, and associates with adverse clinical outcomes. Quantitative assessment of PPFE progression may provide a clinically relevant imaging biomarker to identify individuals at increased risk of respiratory morbidity within LCS programmes.
Association of Radiologic PPFE Change with Mortality in Lung Cancer Screening Cohorts
Mar 10, 2026Background: Pleuroparenchymal fibroelastosis (PPFE) is an upper lobe predominant fibrotic lung abnormality associated with increased mortality in established interstitial lung disease. However, the clinical significance of radiologic PPFE progression in lung cancer screening populations remains unclear. We investigated whether longitudinal change in PPFE quantified on low dose CT independently associates with mortality and respiratory morbidity. Methods: We analysed longitudinal low-dose CT scans and clinical data from two lung cancer screening studies: the National Lung Screening Trial (NLST; n=7980) and the SUMMIT study (n=8561). An automated algorithm quantified PPFE volume on baseline and follow up scans. Annualised change in PPFE (dPPFE) was derived and dichotomised using a distribution based threshold to define progressive PPFE. Associations between dPPFE and mortality were evaluated using Cox proportional hazards models adjusted for demographic and clinical variables. In the SUMMIT cohort, dPPFE was also examined in relation to clinical outcomes. Findings: dPPFE independently associated with mortality in both cohorts (NLST: HR 1.25, 95% CI 1.01-1.56, p=0.042; SUMMIT: HR 3.14, 95% CI 1.66-5.97, p<0.001). Kaplan-Meier curves showed reduced survival among participants with progressive PPFE in both cohorts. In SUMMIT, dPPFE was associated with higher respiratory admissions (IRR 2.79, p<0.001), increased antibiotic and steroid use (IRR 1.55, p=0.010), and a trend towards higher mMRC scores (OR 1.40, p=0.055). Interpretation: Radiologic PPFE progression independently associates with mortality across two large lung cancer screening cohorts and with adverse clinical outcomes. Quantitative assessment of PPFE progression may provide a clinically relevant imaging biomarker for identifying individuals at increased respiratory risk within screening programmes.
The effect of variable labels on deep learning models trained to predict breast density
Oct 08, 2022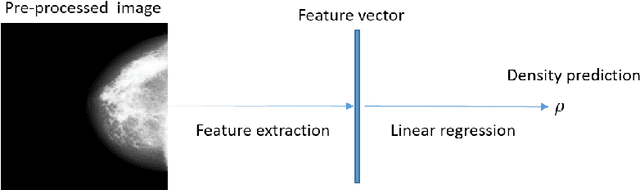
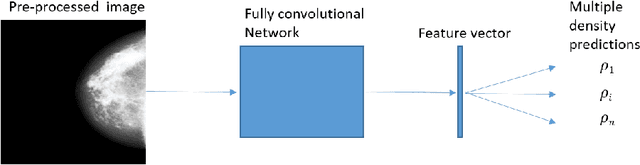
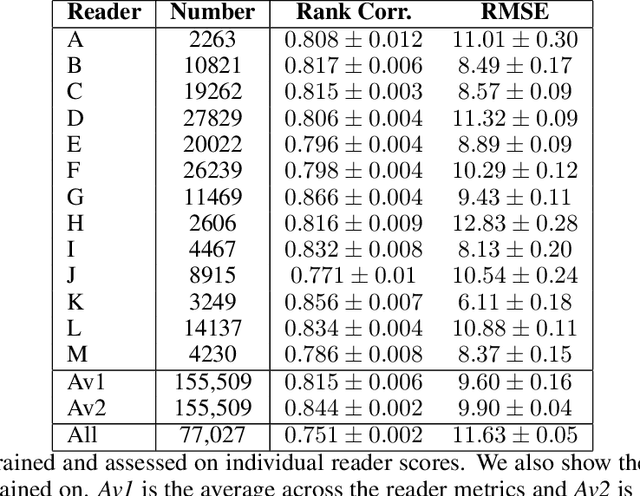
Purpose: High breast density is associated with reduced efficacy of mammographic screening and increased risk of developing breast cancer. Accurate and reliable automated density estimates can be used for direct risk prediction and passing density related information to further predictive models. Expert reader assessments of density show a strong relationship to cancer risk but also inter-reader variation. The effect of label variability on model performance is important when considering how to utilise automated methods for both research and clinical purposes. Methods: We utilise subsets of images with density labels to train a deep transfer learning model which is used to assess how label variability affects the mapping from representation to prediction. We then create two end-to-end deep learning models which allow us to investigate the effect of label variability on the model representation formed. Results: We show that the trained mappings from representations to labels are altered considerably by the variability of reader scores. Training on labels with distribution variation removed causes the Spearman rank correlation coefficients to rise from $0.751\pm0.002$ to either $0.815\pm0.006$ when averaging across readers or $0.844\pm0.002$ when averaging across images. However, when we train different models to investigate the representation effect we see little difference, with Spearman rank correlation coefficients of $0.846\pm0.006$ and $0.850\pm0.006$ showing no statistically significant difference in the quality of the model representation with regard to density prediction. Conclusions: We show that the mapping between representation and mammographic density prediction is significantly affected by label variability. However, the effect of the label variability on the model representation is limited.