 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeFluorescence Image Histology Pattern Transformation using Image Style Transfer
May 15, 2019
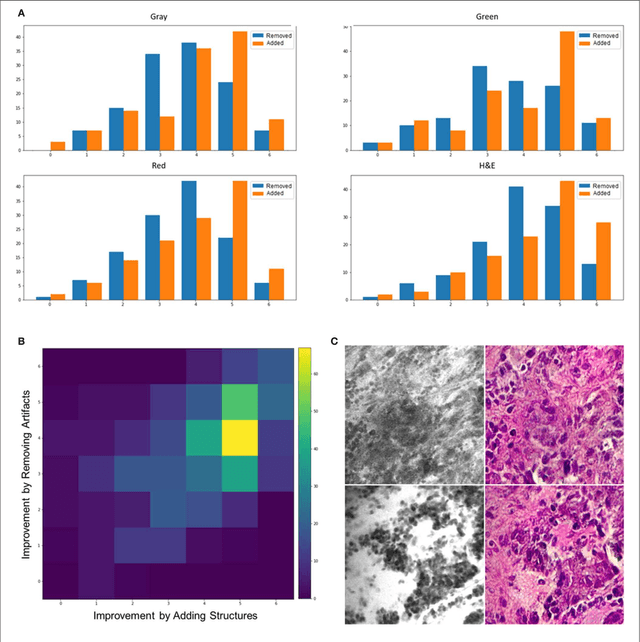
Confocal laser endomicroscopy (CLE) allow on-the-fly in vivo intraoperative imaging in a discreet field of view, especially for brain tumors, rather than extracting tissue for examination ex vivo with conventional light microscopy. Fluorescein sodium-driven CLE imaging is more interactive, rapid, and portable than conventional hematoxylin and eosin (H&E)-staining. However, it has several limitations: CLE images may be contaminated with artifacts (motion, red blood cells, noise), and neuropathologists are mainly trained on colorful stained histology slides like H&E while the CLE images are gray. To improve the diagnostic quality of CLE, we used a micrograph of an H&E slide from a glioma tumor biopsy and image style transfer, a neural network method for integrating the content and style of two images. This was done through minimizing the deviation of the target image from both the content (CLE) and style (H&E) images. The style transferred images were assessed and compared to conventional H&E histology by neurosurgeons and a neuropathologist who then validated the quality enhancement in 100 pairs of original and transformed images. Average reviewers' score on test images showed 84 out of 100 transformed images had fewer artifacts and more noticeable critical structures compared to their original CLE form. By providing images that are more interpretable than the original CLE images and more rapidly acquired than H&E slides, the style transfer method allows a real-time, cellular-level tissue examination using CLE technology that closely resembles the conventional appearance of H&E staining and may yield better diagnostic recognition than original CLE grayscale images.
Prospects for Theranostics in Neurosurgical Imaging: Empowering Confocal Laser Endomicroscopy Diagnostics via Deep Learning
Aug 18, 2018
Confocal laser endomicroscopy (CLE) is an advanced optical fluorescence imaging technology that has the potential to increase intraoperative precision, extend resection, and tailor surgery for malignant invasive brain tumors because of its subcellular dimension resolution. Despite its promising diagnostic potential, interpreting the gray tone fluorescence images can be difficult for untrained users. In this review, we provide a detailed description of bioinformatical analysis methodology of CLE images that begins to assist the neurosurgeon and pathologist to rapidly connect on-the-fly intraoperative imaging, pathology, and surgical observation into a conclusionary system within the concept of theranostics. We present an overview and discuss deep learning models for automatic detection of the diagnostic CLE images and discuss various training regimes and ensemble modeling effect on the power of deep learning predictive models. Two major approaches reviewed in this paper include the models that can automatically classify CLE images into diagnostic/nondiagnostic, glioma/nonglioma, tumor/injury/normal categories and models that can localize histological features on the CLE images using weakly supervised methods. We also briefly review advances in the deep learning approaches used for CLE image analysis in other organs. Significant advances in speed and precision of automated diagnostic frame selection would augment the diagnostic potential of CLE, improve operative workflow and integration into brain tumor surgery. Such technology and bioinformatics analytics lend themselves to improved precision, personalization, and theranostics in brain tumor treatment.
Weakly-Supervised Learning-Based Feature Localization in Confocal Laser Endomicroscopy Glioma Images
Aug 18, 2018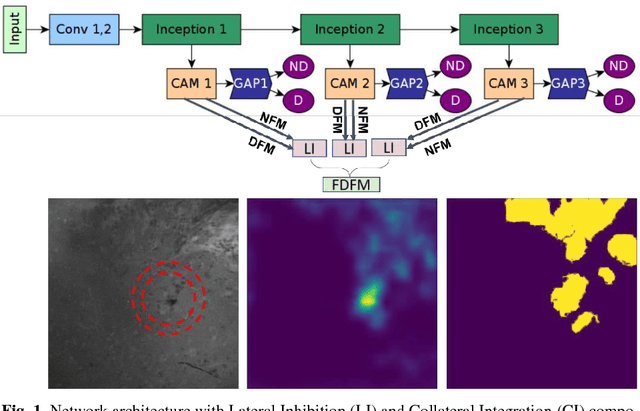
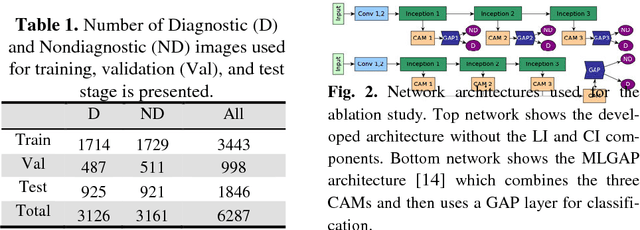
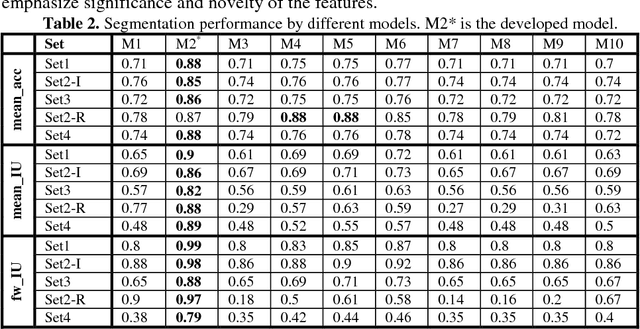
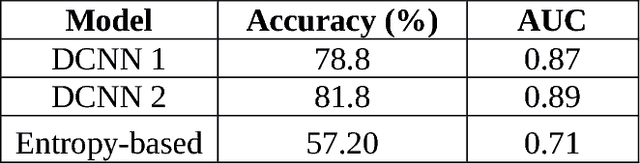
Confocal Laser Endomicroscope (CLE) is a novel handheld fluorescence imaging device that has shown promise for rapid intraoperative diagnosis of brain tumor tissue. Currently CLE is capable of image display only and lacks an automatic system to aid the surgeon in analyzing the images. The goal of this project was to develop a computer-aided diagnostic approach for CLE imaging of human glioma with feature localization function. Despite the tremendous progress in object detection and image segmentation methods in recent years, most of such methods require large annotated datasets for training. However, manual annotation of thousands of histopathological images by physicians is costly and time consuming. To overcome this problem, we propose a Weakly-Supervised Learning (WSL)-based model for feature localization that trains on image-level annotations, and then localizes incidences of a class-of-interest in the test image. We developed a novel convolutional neural network for diagnostic features localization from CLE images by employing a novel multiscale activation map that is laterally inhibited and collaterally integrated. To validate our method, we compared proposed model's output to the manual annotation performed by four neurosurgeons on test images. Proposed model achieved 88% mean accuracy and 86% mean intersection over union on intermediate features and 87% mean accuracy and 88% mean intersection over union on restrictive fine features, while outperforming other state of the art methods tested. This system can improve accuracy and efficiency in characterization of CLE images of glioma tissue during surgery, augment intraoperative decision-making process regarding tumor margin and affect resection rates.
Improving utility of brain tumor confocal laser endomicroscopy: objective value assessment and diagnostic frame detection with convolutional neural networks
Jan 06, 2018Confocal laser endomicroscopy (CLE), although capable of obtaining images at cellular resolution during surgery of brain tumors in real time, creates as many non-diagnostic as diagnostic images. Non-useful images are often distorted due to relative motion between probe and brain or blood artifacts. Many images, however, simply lack diagnostic features immediately informative to the physician. Examining all the hundreds or thousands of images from a single case to discriminate diagnostic images from nondiagnostic ones can be tedious. Providing a real-time diagnostic value assessment of images (fast enough to be used during the surgical acquisition process and accurate enough for the pathologist to rely on) to automatically detect diagnostic frames would streamline the analysis of images and filter useful images for the pathologist/surgeon. We sought to automatically classify images as diagnostic or non-diagnostic. AlexNet, a deep-learning architecture, was used in a 4-fold cross validation manner. Our dataset includes 16,795 images (8572 nondiagnostic and 8223 diagnostic) from 74 CLE-aided brain tumor surgery patients. The ground truth for all the images is provided by the pathologist. Average model accuracy on test data was 91% overall (90.79 % accuracy, 90.94 % sensitivity and 90.87 % specificity). To evaluate the model reliability we also performed receiver operating characteristic (ROC) analysis yielding 0.958 average for the area under ROC curve (AUC). These results demonstrate that a deeply trained AlexNet network can achieve a model that reliably and quickly recognizes diagnostic CLE images.
* SPIE Medical Imaging: Computer-Aided Diagnosis 2017
Convolutional Neural Networks: Ensemble Modeling, Fine-Tuning and Unsupervised Semantic Localization for Intraoperative CLE Images
Oct 23, 2017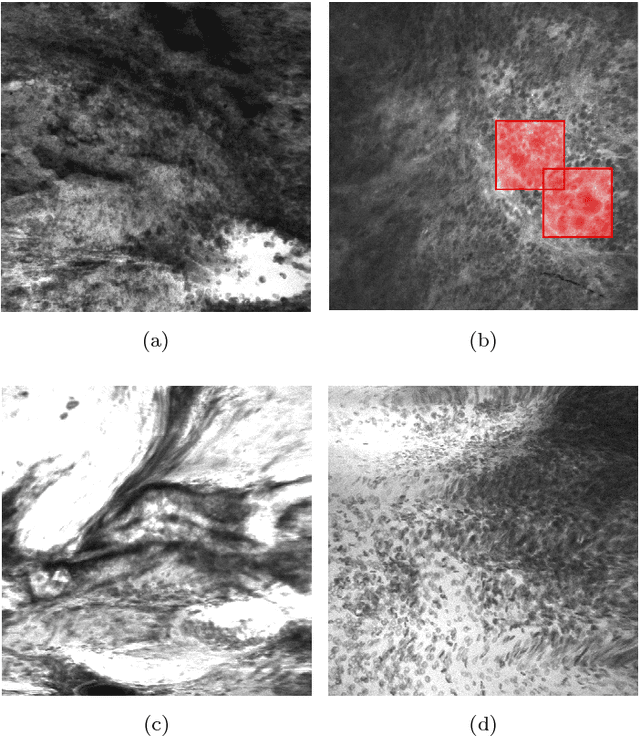
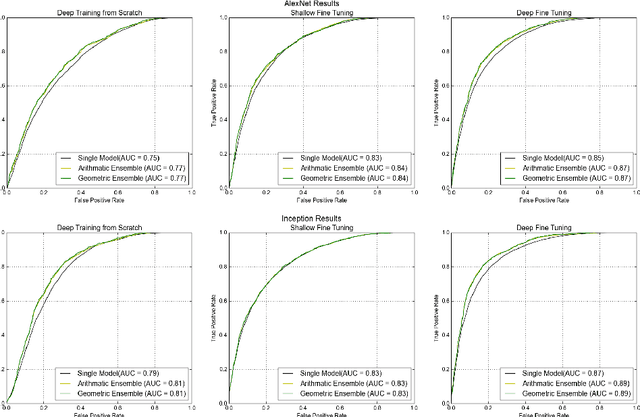
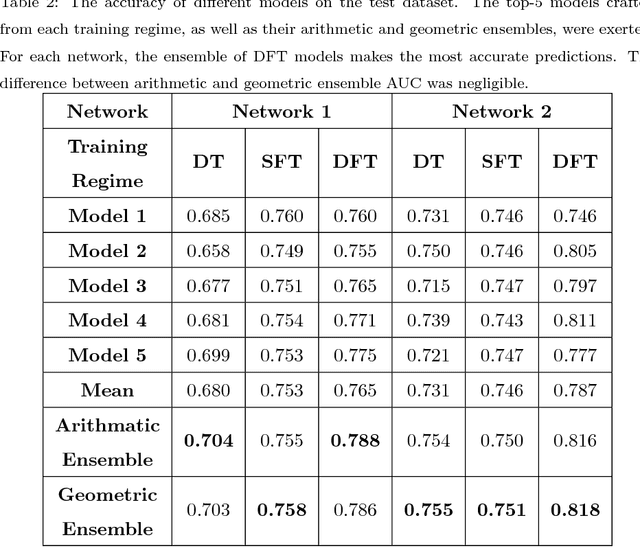
Confocal laser endomicroscopy (CLE) is an advanced optical fluorescence technology undergoing assessment for applications in brain tumor surgery. Despite its promising potential, interpreting the unfamiliar gray tone images of fluorescent stains can be difficult. Many of the CLE images can be distorted by motion, extremely low or high fluorescence signal, or obscured by red blood cell accumulation, and these can be interpreted as nondiagnostic. However, just one neat CLE image might suffice for intraoperative diagnosis of the tumor. While manual examination of thousands of nondiagnostic images during surgery would be impractical, this creates an opportunity for a model to select diagnostic images for the pathologists or surgeon's review. In this study, we sought to develop a deep learning model to automatically detect the diagnostic images using a manually annotated dataset, and we employed a patient-based nested cross-validation approach to explore generalizability of the model. We explored various training regimes: deep training, shallow fine-tuning, and deep fine-tuning. Further, we investigated the effect of ensemble modeling by combining the top-5 single models crafted in the development phase. We localized histological features from diagnostic CLE images by visualization of shallow and deep neural activations. Our inter-rater experiment results confirmed that our ensemble of deeply fine-tuned models achieved higher agreement with the ground truth than the other observers. With the speed and precision of the proposed method (110 images/second; 85% on the gold standard test subset), it has potential to be integrated into the operative workflow in the brain tumor surgery.