 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMulti-planar 2D-U-Net Segmentation of 3D-CT Abdominal Organs augmented by Spatial Occurrence Maps
Jun 05, 2026This work proposes a lightweight 2D-U-Net-based framework for segmenting five abdominal organs in large field-of-view 3D CT scans. The method combines coarse-to-fine segmentation, predictions from multiple anatomical planes, and additional fuzzy 3D spatial maps that provide anatomical location cues to improve segmentation accuracy. We combine multi-planar 2D-U-Net models augmented by a spatial occurrence map. The approach involves two main stages. First, the abdominal volume of interest region is detected by traversing the whole scan axially with a 2D-U-Net and determining the x-y-z-minimum and -maximum extents of the 5 abdominal organs of interest. Second, we use spatial occurrence maps to enhance our multi-planar 2D-U-net architecture inside the bounds from the former stage. The method is evaluated on 80 CT scans from various public sources. The results show Dice improvements of about 4% at maximum compared to the same model trained without spatial occurrence maps.
SC-MFJ: A Simple Haptic Quality Metric for Medical Image Segmentation
Jun 04, 2026Standard segmentation metrics such as Dice and Hausdorff distance measure geometric overlap but say nothing about whether a segmented surface is suitable for haptic rendering in surgical simulation. We propose SC-MFJ (Surface-Constrained Mean Force Jerk), a simple, inexpensive metric that samples a segmented organ surface with many short virtual stylus walks and measures how jerky the resulting contact forces are. The metric is computed from existing segmentation outputs and uses roughly one minute of CPU time per case. We evaluate three pancreas CT segmentation approaches-binary nnU-Net output, Gaussian-smoothed output, and learned signed distance function (SDF) regression-across 80 cases in five-fold cross-validation. SC-MFJ reveals a 147x gap in haptic quality between the raw binary baseline and simple Gaussian post-processing, a difference entirely invisible to Dice and HD95. It also shows that learned SDF regression, despite requiring full model retraining, produces more variable haptic quality than Gaussian smoothing, with a case-level standard deviation of 168 N/s2 compared with 22 N/s2 for Gaussian. A second evaluation on the LiTS liver dataset (131 cases) confirms the generality of these findings: the binary-to-Gaussian gap widens to 189x, and Gaussian smoothing again produces consistently low force jerk across all folds. Our results suggest that for haptic simulation applications, a one-line post-processing step may be sufficient, and that a cheap metric like SC-MFJ can flag problems that geometric metrics miss.
Comparison of 2D vs. 3D U-Net Organ Segmentation in abdominal 3D CT images
Jul 08, 2021
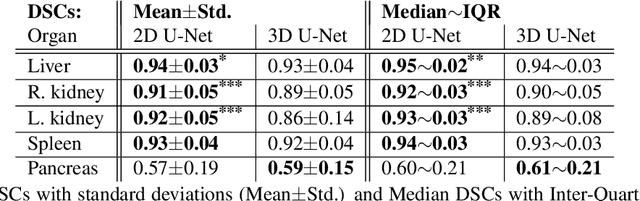

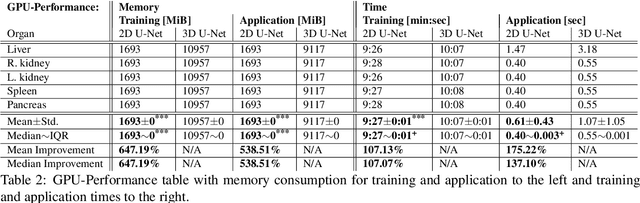
A two-step concept for 3D segmentation on 5 abdominal organs inside volumetric CT images is presented. First each relevant organ's volume of interest is extracted as bounding box. The extracted volume acts as input for a second stage, wherein two compared U-Nets with different architectural dimensions re-construct an organ segmentation as label mask. In this work, we focus on comparing 2D U-Nets vs. 3D U-Net counterparts. Our initial results indicate Dice improvements of about 6\% at maximum. In this study to our surprise, liver and kidneys for instance were tackled significantly better using the faster and GPU-memory saving 2D U-Nets. For other abdominal key organs, there were no significant differences, but we observe highly significant advantages for the 2D U-Net in terms of GPU computational efforts for all organs under study.
* 9 pages, 6 figure, 2 tables
3D Bounding Box Detection in Volumetric Medical Image Data: A Systematic Literature Review
Dec 10, 2020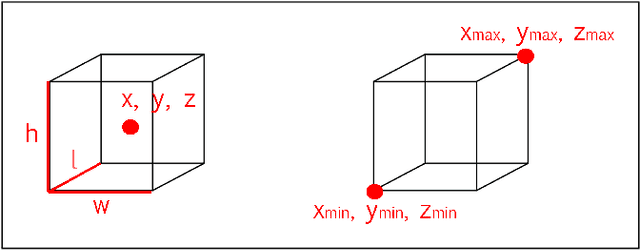
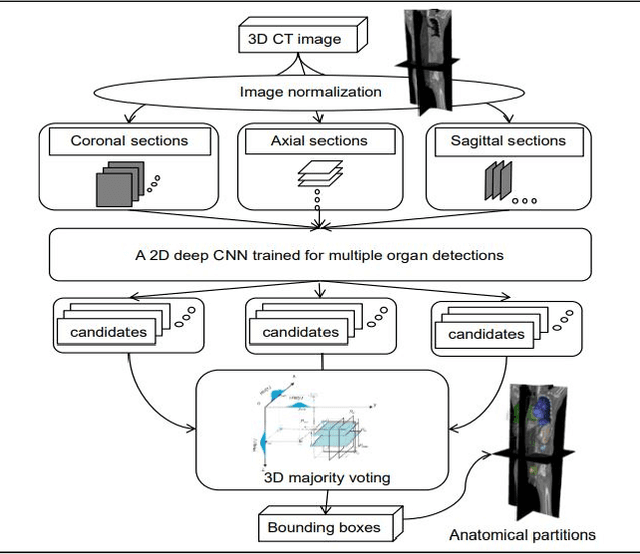
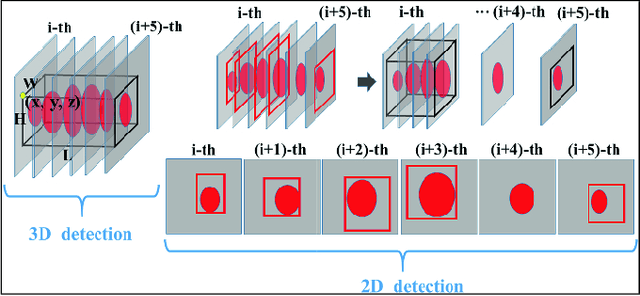
This paper discusses current methods and trends for 3D bounding box detection in volumetric medical image data. For this purpose, an overview of relevant papers from recent years is given. 2D and 3D implementations are discussed and compared. Multiple identified approaches for localizing anatomical structures are presented. The results show that most research recently focuses on Deep Learning methods, such as Convolutional Neural Networks vs. methods with manual feature engineering, e.g. Random-Regression-Forests. An overview of bounding box detection options is presented and helps researchers to select the most promising approach for their target objects.
* 10 pages, 5 figures, 1 table
Robust GPU-based Virtual Reality Simulation of Radio Frequency Ablations for Various Needle Geometries and Locations
Jul 11, 2019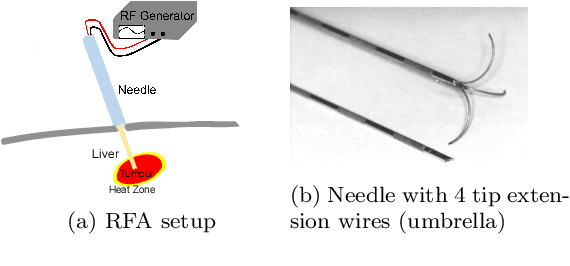

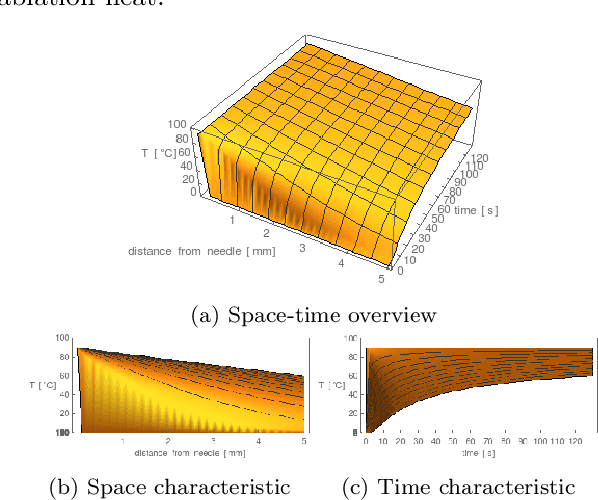
Purpose: Radio-frequency ablations play an important role in the therapy of malignant liver lesions. The navigation of a needle to the lesion poses a challenge for both the trainees and intervening physicians. Methods: This publication presents a new GPU-based, accurate method for the simulation of radio-frequency ablations for lesions at the needle tip in general and for an existing visuo-haptic 4D VR simulator. The method is implemented real-time capable with Nvidia CUDA. Results: It performs better than a literature method concerning the theoretical characteristic of monotonic convergence of the bioheat PDE and a in vitro gold standard with significant improvements (p < 0.05) in terms of Pearson correlations. It shows no failure modes or theoretically inconsistent individual simulation results after the initial phase of 10 seconds. On the Nvidia 1080 Ti GPU it achieves a very high frame rendering performance of >480 Hz. Conclusion: Our method provides a more robust and safer real-time ablation planning and intraoperative guidance technique, especially avoiding the over-estimation of the ablated tissue death zone, which is risky for the patient in terms of tumor recurrence. Future in vitro measurements and optimization shall further improve the conservative estimate.
* 18 pages, 14 figures, 1 table, 2 algorithms, 2 movies
Genaue modellbasierte Identifikation von gynäkologischen Katheterpfaden für die MRT-bildgestützte Brachytherapie
Mar 10, 2018German text, english abstract: Mortality in gynecologic cancers, including cervical, ovarian, vaginal and vulvar cancers, is more than 6% internationally [1]. In many countries external radiotherapy is supplemented by brachytherapy with high locally administered doses as standard. The superior ability of magnetic resonance imaging (MRI) to differentiate soft tissue has led to an increasing use of this imaging technique in the intraoperative planning and implementation of brachytherapy. A technical challenge associated with the use of MRI imaging for brachytherapy - in contrast to computed tomography (CT) imaging - is the dark-diffuse appearance and thus difficult identification of the catheter paths in the resulting images. This problem is addressed by the precise method described herein of tracing the catheters from the catheter tip. The average identification time for a single catheter path was three seconds on a standard PC. Segmentation time, accuracy and precision are promising indicators of the value of this method for the clinical application of image-guided gynecological brachytherapy. After surgery (OP), the healthy surrounding tissue of the tumor is usually irradiated. This reduces the risk of leaving behind residual cells that would likely cause a recurrence of the cancer or the formation of metastases - secondary tumors elsewhere in the body. In the case of a tumor on the cervix or prostate, the operation is minimally invasive, ie. the removal of the cancer and the irradiation are performed cost-effectively and risk-avoiding by keyhole surgery instead of open surgery.
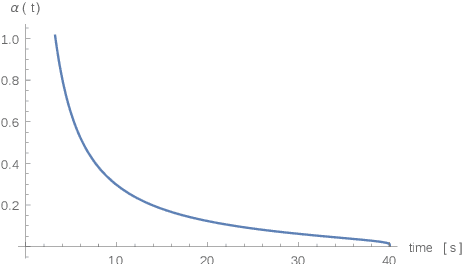
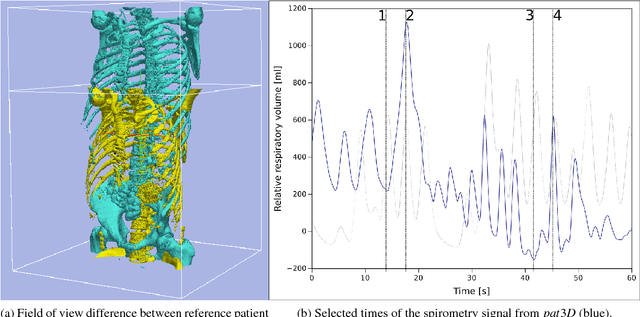
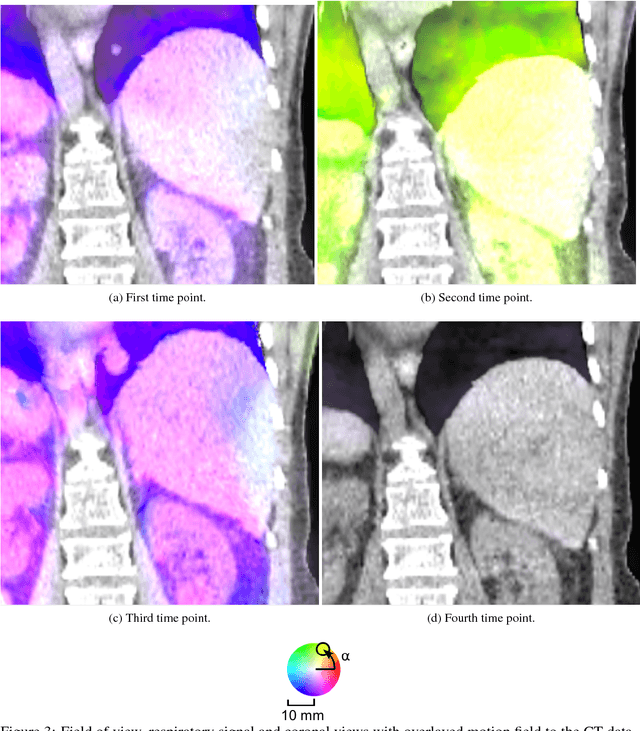
Population-based Respiratory 4D Motion Atlas Construction and its Application for VR Simulations of Liver Punctures
Dec 22, 2017Virtual reality (VR) training simulators of liver needle insertion in the hepatic area of breathing virtual patients currently need 4D data acquisitions as a prerequisite. Here, first a population-based breathing virtual patient 4D atlas can be built and second the requirement of a dose-relevant or expensive acquisition of a 4D data set for a new static 3D patient can be mitigated by warping the mean atlas motion. The breakthrough contribution of this work is the construction and reuse of population-based learned 4D motion models.
Interpatient Respiratory Motion Model Transfer for Virtual Reality Simulations of Liver Punctures
Aug 02, 2017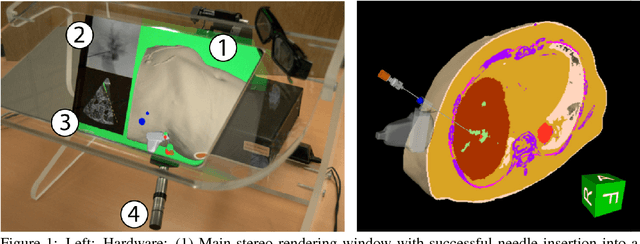
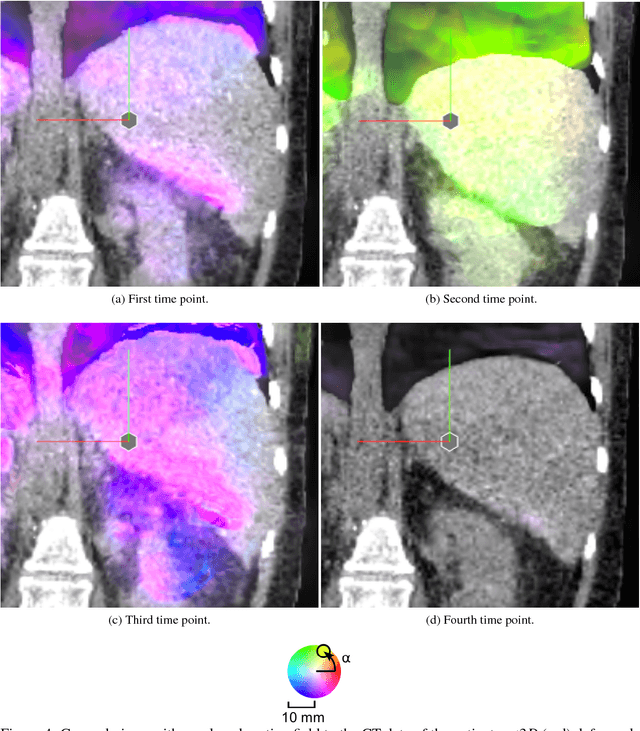
Current virtual reality (VR) training simulators of liver punctures often rely on static 3D patient data and use an unrealistic (sinusoidal) periodic animation of the respiratory movement. Existing methods for the animation of breathing motion support simple mathematical or patient-specific, estimated breathing models. However with personalized breathing models for each new patient, a heavily dose relevant or expensive 4D data acquisition is mandatory for keyframe-based motion modeling. Given the reference 4D data, first a model building stage using linear regression motion field modeling takes place. Then the methodology shown here allows the transfer of existing reference respiratory motion models of a 4D reference patient to a new static 3D patient. This goal is achieved by using non-linear inter-patient registration to warp one personalized 4D motion field model to new 3D patient data. This cost- and dose-saving new method is shown here visually in a qualitative proof-of-concept study.
* World Society for Computer Graphics - WSCG 2017 publication, 9 pages, 5 figures, 1 movie online
A New 3D Segmentation Technique for QCT Scans of the Lumbar Spine to Determine BMD and Vertebral Geometry
May 19, 2017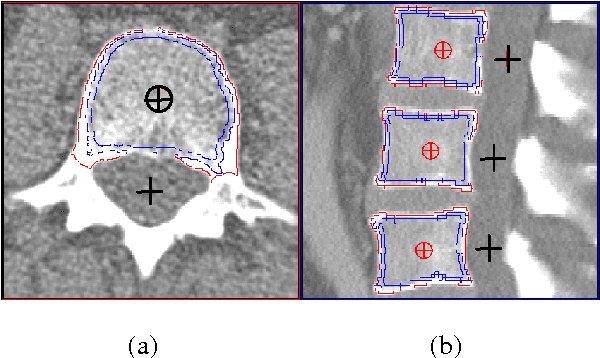
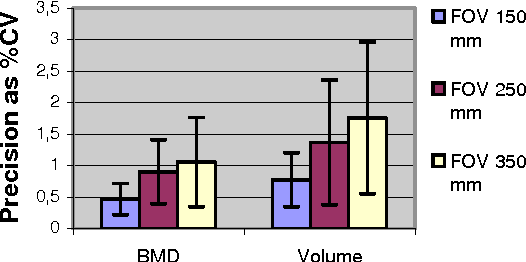
Quantitative computed tomography (QCT) is a standard method to determine bone mineral density (BMD) in the spine. Traditionally single 8 - 10 mm thick slices have been analyzed only. Current spiral CT scanners provide true 3D acquisition schemes allowing for a more differential BMD analysis and an assessment of geometric parameters, which may improve fracture prediction. We developed a novel 3D segmentation approach that combines deformable balloons, multi seeded volume growing, and dedicated morphological operations to extract the vertebral bodies. An anatomy-oriented coordinate system attached automatically to each vertebra is used to define volumes of interest. We analyzed intra-operator precision of the segmentation procedure using abdominal scans from 10 patients (60 mAs, 120 kV, slice thickness 1mm, B40s, Siemens Sensation 16). Our new segmentation method shows excellent precision errors in the order of < 1 % for BMD and < 2 % for volume.
A New 3D Method to Segment the Lumbar Vertebral Bodies and to Determine Bone Mineral Density and Geometry
May 19, 2017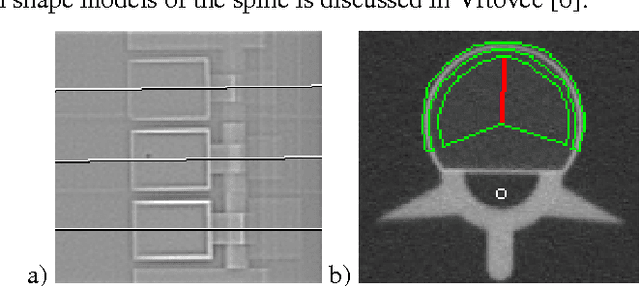
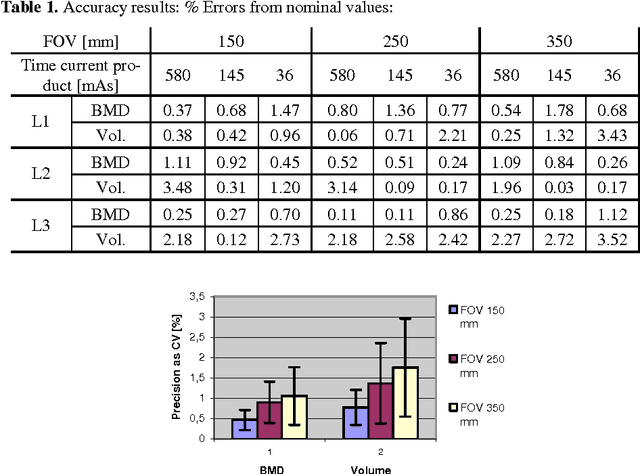
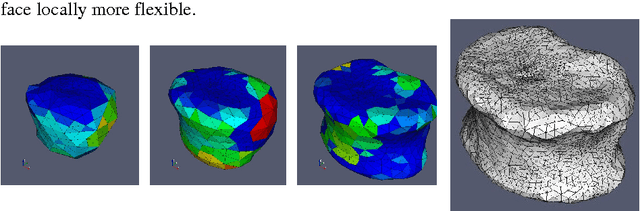
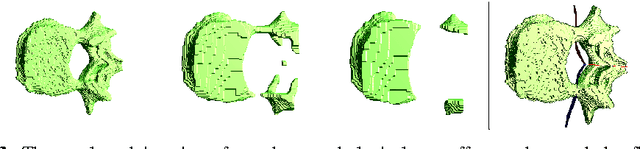
In this paper we present a new 3D segmentation approach for the vertebrae of the lower thoracic and the lumbar spine in spiral computed tomography datasets. We implemented a multi-step procedure. Its main components are deformable models, volume growing, and morphological operations. The performance analysis that included an evaluation of accuracy using the European Spine Phantom, and of intra-operator precision using clinical CT datasets from 10 patients highlight the potential for clinical use. The intra-operator precision of the segmentation procedure was better than 1% for Bone Mineral Density (BMD) and better than 1.8% for volume. The long-term goal of this work is to enable better fracture prediction and improved patient monitoring in the field of osteoporosis. A true 3D segmentation also enables an accurate measurement of geometrical parameters that can augment the classical measurement of BMD.