 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeTreatment Response Optimized Clinical Decision Support AI System via Digital Twin Simulation
Jun 16, 2026Clinical decision support AI systems (CDSASs) must adapt to evolving patient conditions in real-time while adhering to strict safety constraints. We present an online adaptive framework that integrates Treatment Effect (TE) estimation to quantify clinical benefits, a patient Digital Twin (DT) to simulate treatment trajectories, and Reinforcement Learning (RL) for sequential decision-making. The AI system is initially trained on historical medical records and operates in a continuous learning loop. To ensure safety, a rule-based module monitors vital signs and blocks contraindicated treatments. Cases with strong internal model disagreement are flagged for clinician review, simulated in our experiments via a pre-trained outcome model. We validate our framework using both a synthetic clinical simulator and a real-world ovarian cancer dataset from The Cancer Genome Atlas (TCGA). In both simulated and clinical settings, our method demonstrated superior effectiveness and stability in recommending treatments compared to standard computational baselines. Furthermore, the AI system maintains low latency and requires expert consultation for only a minority of cases in our experimental validation, demonstrating its potential as a safe, clinician-supervised tool for personalized medicine that continuously improves through practical use.
Reinforcement Learning enhanced Online Adaptive Clinical Decision Support via Digital Twin powered Policy and Treatment Effect optimized Reward
Aug 24, 2025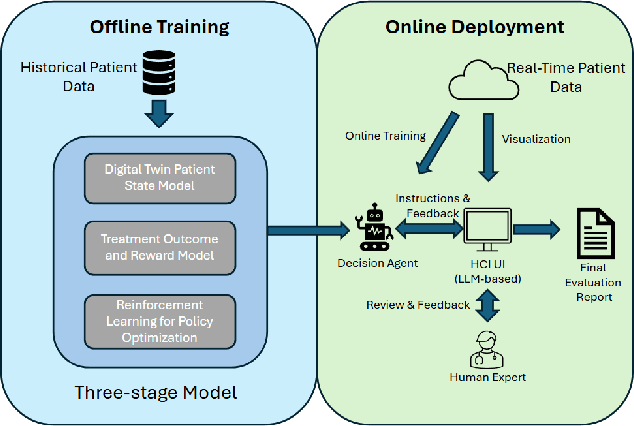
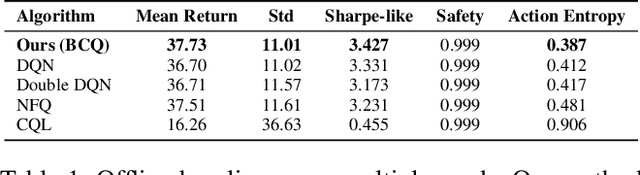
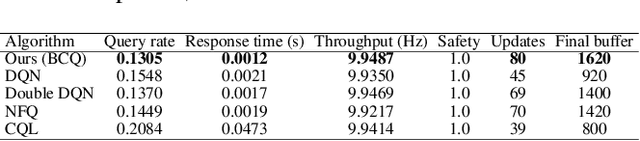
Clinical decision support must adapt online under safety constraints. We present an online adaptive tool where reinforcement learning provides the policy, a patient digital twin provides the environment, and treatment effect defines the reward. The system initializes a batch-constrained policy from retrospective data and then runs a streaming loop that selects actions, checks safety, and queries experts only when uncertainty is high. Uncertainty comes from a compact ensemble of five Q-networks via the coefficient of variation of action values with a $\tanh$ compression. The digital twin updates the patient state with a bounded residual rule. The outcome model estimates immediate clinical effect, and the reward is the treatment effect relative to a conservative reference with a fixed z-score normalization from the training split. Online updates operate on recent data with short runs and exponential moving averages. A rule-based safety gate enforces vital ranges and contraindications before any action is applied. Experiments in a synthetic clinical simulator show low latency, stable throughput, a low expert query rate at fixed safety, and improved return against standard value-based baselines. The design turns an offline policy into a continuous, clinician-supervised system with clear controls and fast adaptation.
Explainable Counterfactual Reasoning in Depression Medication Selection at Multi-Levels (Personalized and Population)
Aug 24, 2025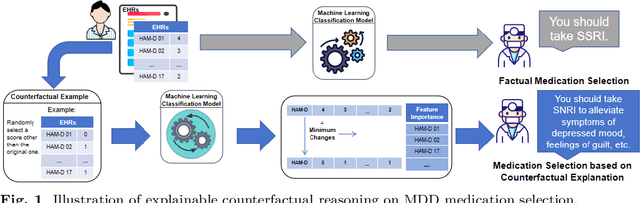
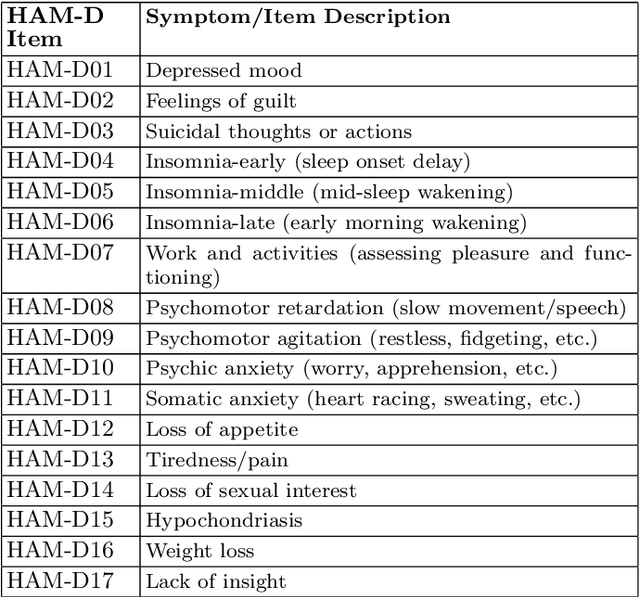
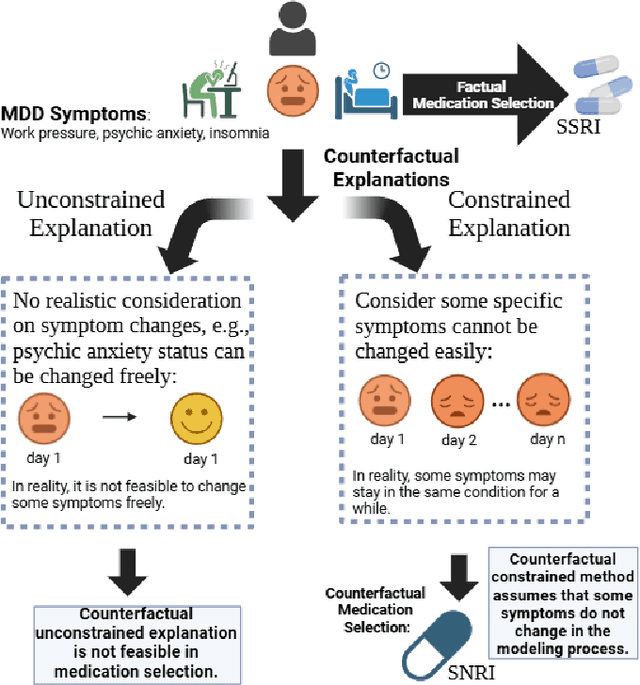
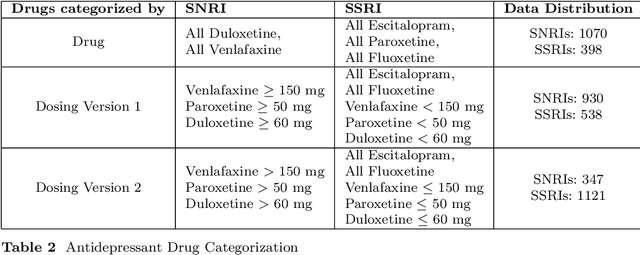
Background: This study investigates how variations in Major Depressive Disorder (MDD) symptoms, quantified by the Hamilton Rating Scale for Depression (HAM-D), causally influence the prescription of SSRIs versus SNRIs. Methods: We applied explainable counterfactual reasoning with counterfactual explanations (CFs) to assess the impact of specific symptom changes on antidepressant choice. Results: Among 17 binary classifiers, Random Forest achieved highest performance (accuracy, F1, precision, recall, ROC-AUC near 0.85). Sample-based CFs revealed both local and global feature importance of individual symptoms in medication selection. Conclusions: Counterfactual reasoning elucidates which MDD symptoms most strongly drive SSRI versus SNRI selection, enhancing interpretability of AI-based clinical decision support systems. Future work should validate these findings on more diverse cohorts and refine algorithms for clinical deployment.