 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDocument Understanding for Healthcare Referrals
Sep 22, 2023Reliance on scanned documents and fax communication for healthcare referrals leads to high administrative costs and errors that may affect patient care. In this work we propose a hybrid model leveraging LayoutLMv3 along with domain-specific rules to identify key patient, physician, and exam-related entities in faxed referral documents. We explore some of the challenges in applying a document understanding model to referrals, which have formats varying by medical practice, and evaluate model performance using MUC-5 metrics to obtain appropriate metrics for the practical use case. Our analysis shows the addition of domain-specific rules to the transformer model yields greatly increased precision and F1 scores, suggesting a hybrid model trained on a curated dataset can increase efficiency in referral management.
Evolutionary Clustering via Message Passing
Dec 27, 2019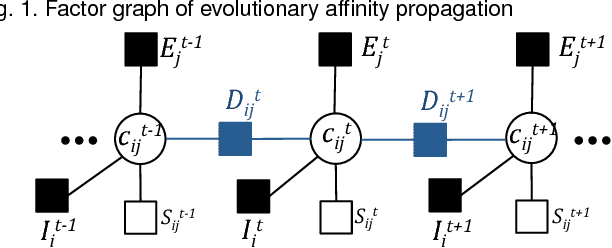
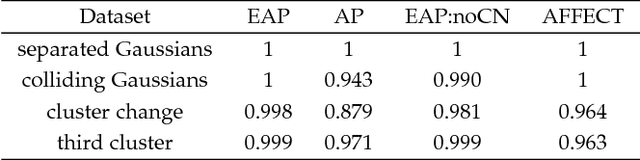
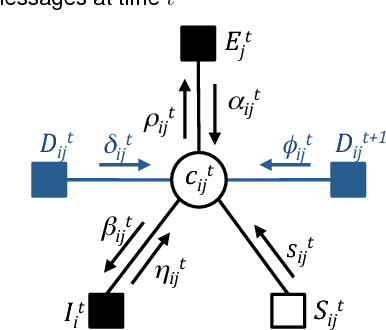
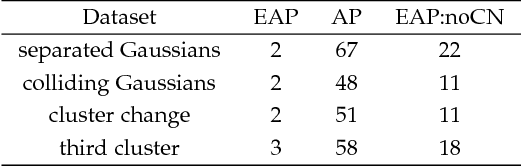
We are often interested in clustering objects that evolve over time and identifying solutions to the clustering problem for every time step. Evolutionary clustering provides insight into cluster evolution and temporal changes in cluster memberships while enabling performance superior to that achieved by independently clustering data collected at different time points. In this paper we introduce evolutionary affinity propagation (EAP), an evolutionary clustering algorithm that groups data points by exchanging messages on a factor graph. EAP promotes temporal smoothness of the solution to clustering time-evolving data by linking the nodes of the factor graph that are associated with adjacent data snapshots, and introduces consensus nodes to enable cluster tracking and identification of cluster births and deaths. Unlike existing evolutionary clustering methods that require additional processing to approximate the number of clusters or match them across time, EAP determines the number of clusters and tracks them automatically. A comparison with existing methods on simulated and experimental data demonstrates effectiveness of the proposed EAP algorithm.
Designing Optimal Mortality Risk Prediction Scores that Preserve Clinical Knowledge
Apr 29, 2015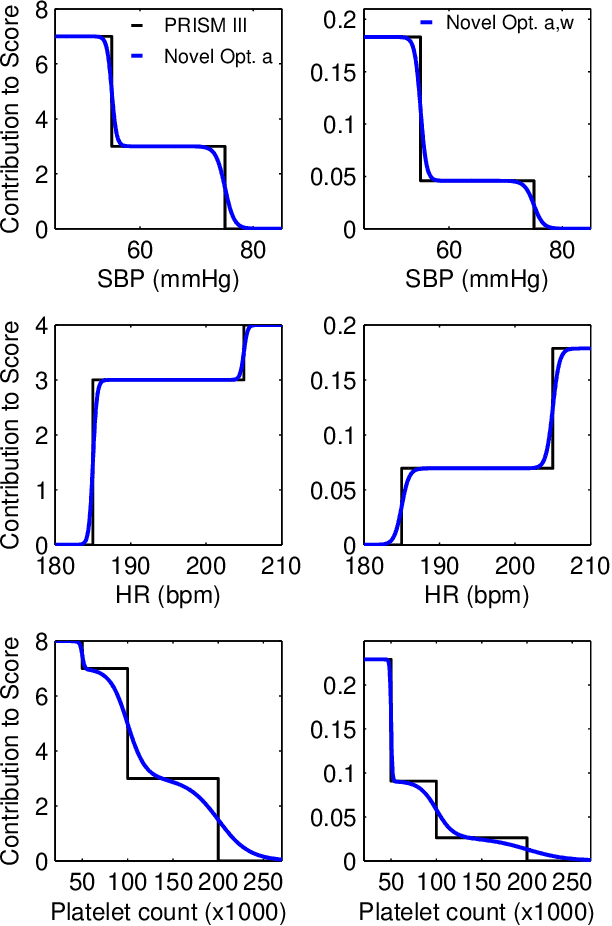
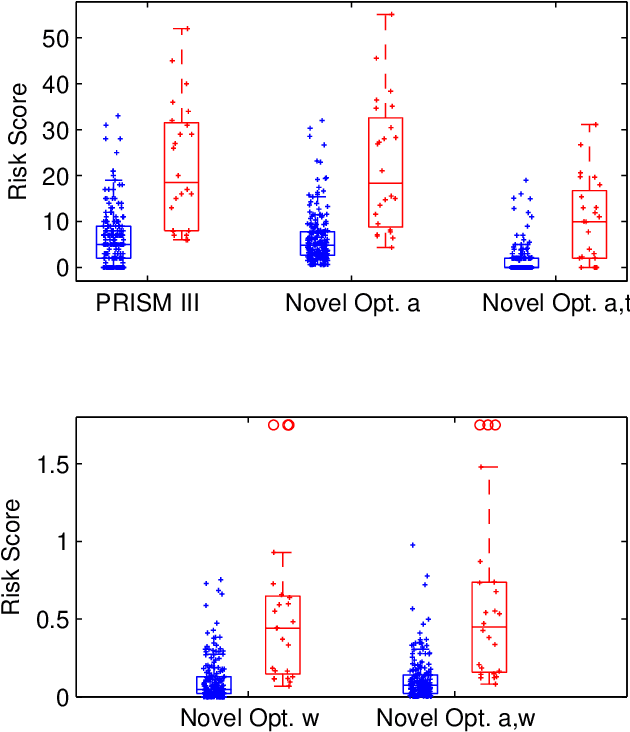
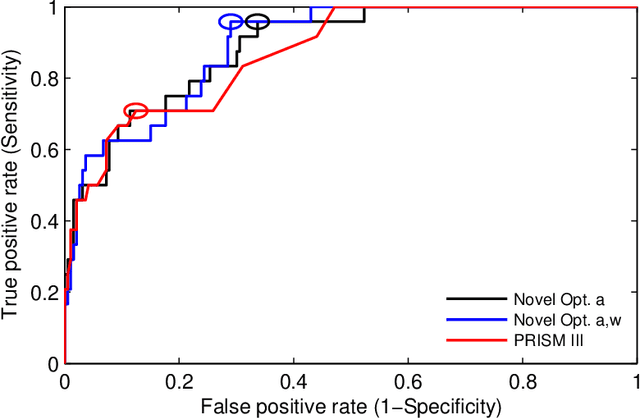
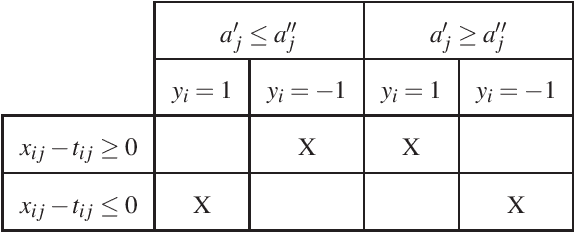
Many in-hospital mortality risk prediction scores dichotomize predictive variables to simplify the score calculation. However, hard thresholding in these additive stepwise scores of the form "add x points if variable v is above/below threshold t" may lead to critical failures. In this paper, we seek to develop risk prediction scores that preserve clinical knowledge embedded in features and structure of the existing additive stepwise scores while addressing limitations caused by variable dichotomization. To this end, we propose a novel score structure that relies on a transformation of predictive variables by means of nonlinear logistic functions facilitating smooth differentiation between critical and normal values of the variables. We develop an optimization framework for inferring parameters of the logistic functions for a given patient population via cyclic block coordinate descent. The parameters may readily be updated as the patient population and standards of care evolve. We tested the proposed methodology on two populations: (1) brain trauma patients admitted to the intensive care unit of the Dell Children's Medical Center of Central Texas between 2007 and 2012, and (2) adult ICU patient data from the MIMIC II database. The results are compared with those obtained by the widely used PRISM III and SOFA scores. The prediction power of a score is evaluated using area under ROC curve, Youden's index, and precision-recall balance in a cross-validation study. The results demonstrate that the new framework enables significant performance improvements over PRISM III and SOFA in terms of all three criteria.