 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeImage Quality in the Era of Artificial Intelligence
Feb 10, 2026Artificial intelligence (AI) is being deployed within radiology at a rapid pace. AI has proven an excellent tool for reconstructing and enhancing images that appear sharper, smoother, and more detailed, can be acquired more quickly, and allowing clinicians to review them more rapidly. However, incorporation of AI also introduces new failure modes and can exacerbate the disconnect between perceived quality of an image and information content of that image. Understanding the limitations of AI-enabled image reconstruction and enhancement is critical for safe and effective use of the technology. Hence, the purpose of this communication is to bring awareness to limitations when AI is used to reconstruct or enhance a radiological image, with the goal of enabling users to reap benefits of the technology while minimizing risks.
Deep learning achieves radiologist-level performance of tumor segmentation in breast MRI
Sep 21, 2020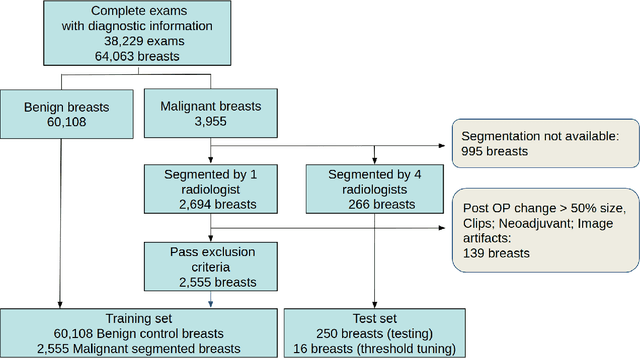
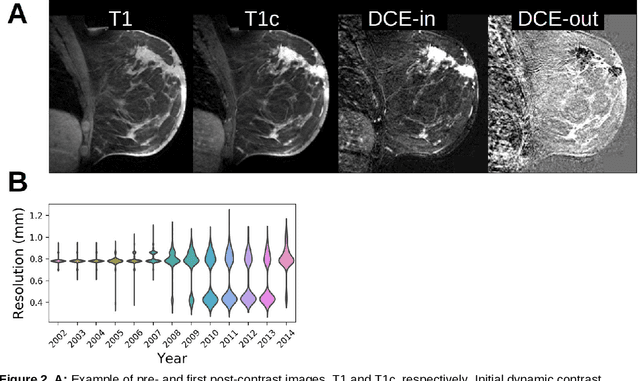
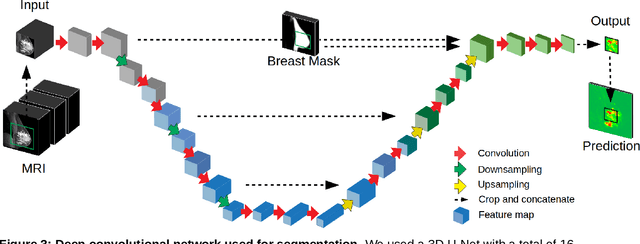
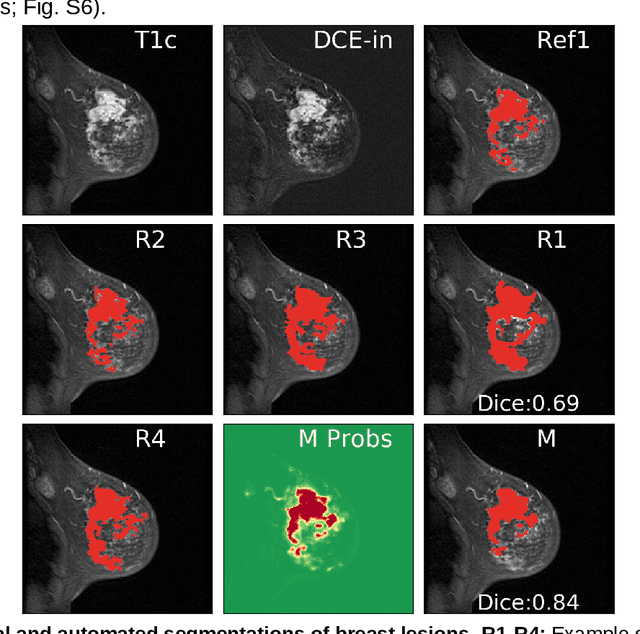
Purpose: The goal of this research was to develop a deep network architecture that achieves fully-automated radiologist-level segmentation of breast tumors in MRI. Materials and Methods: We leveraged 38,229 clinical MRI breast exams collected retrospectively from women aged 12-94 (mean age 54) who presented between 2002 and 2014 at a single clinical site. The training set for the network consisted of 2,555 malignant breasts that were segmented in 2D by experienced radiologists, as well as 60,108 benign breasts that served as negative controls. The test set consisted of 250 exams with tumors segmented independently by four radiologists. We selected among several 3D deep convolutional neural network architectures, input modalities and harmonization methods. The outcome measure was the Dice score for 2D segmentation, and was compared between the network and radiologists using the Wilcoxon signed-rank test and the TOST procedure. Results: The best-performing network on the training set was a volumetric U-Net with contrast enhancement dynamic as input and with intensity normalized for each exam. In the test set the median Dice score of this network was 0.77. The performance of the network was equivalent to that of the radiologists (TOST procedure with radiologist performance of 0.69-0.84 as equivalence bounds: p = 5e-10 and p = 2e-5, respectively; N = 250) and compares favorably with published state of the art (0.6-0.77). Conclusion: When trained on a dataset of over 60 thousand breasts, a volumetric U-Net performs as well as expert radiologists at segmenting malignant breast lesions in MRI.