 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDesign to automate the detection and counting of Tuberculosis bacilli
May 24, 2021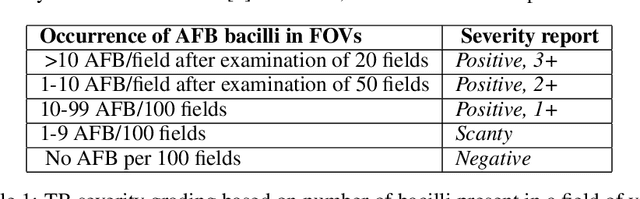
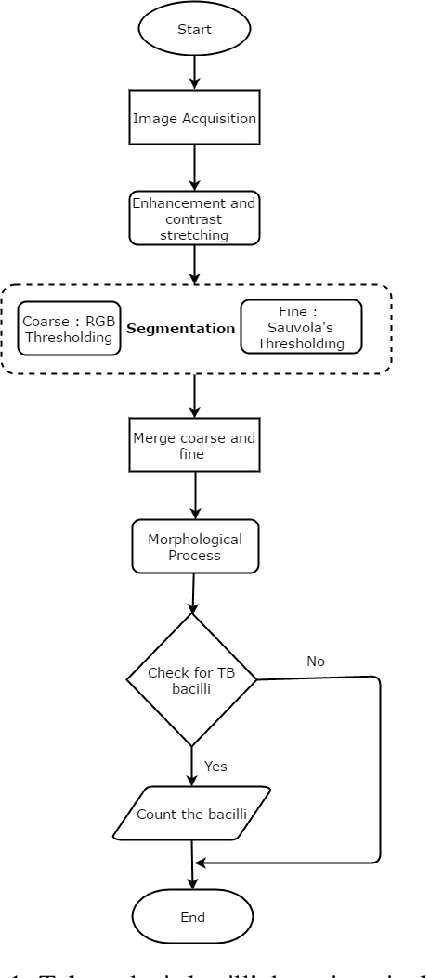
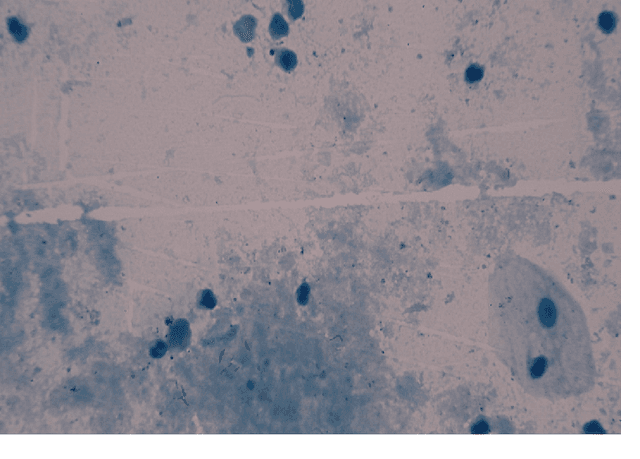
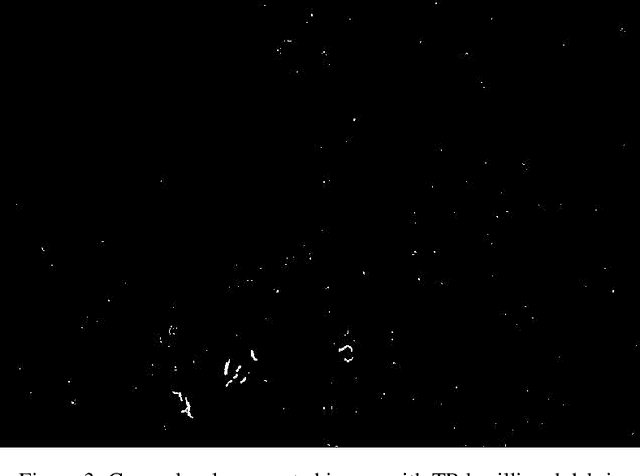
Tuberculosis is a contagious disease which is one of the leading causes of death, globally. The general diagnosis methods for tuberculosis include microscopic examination, tuberculin skin test, culture method, enzyme linked immunosorbent assay (ELISA) and electronic nose system. World Health Organization (WHO) recommends standard microscopic examination for early diagnosis of tuberculosis. In microscopy, the technician examines field of views (FOVs) in sputum smear for presence of any TB bacilli and counts the number of TB bacilli per FOV to report the level of severity. This process is time consuming with an increased concentration for an experienced staff to examine a single sputum smear. The examination demands for skilled technicians in high-prevalence countries which may lead to overload, fatigue and diminishes the quality of microscopy. Thus, a computer assisted system is proposed and designed for the detection of tuberculosis bacilli to assist pathologists with increased sensitivity and specificity. The manual efforts in detecting and counting the number of TB bacilli is greatly minimized. The system obtains Ziehl-Neelsen stained microscopic images from conventional microscope at 100x magnification and passes the data to the detection system. Initially the segmentation of TB bacilli was done using RGB thresholding and Sauvola's adaptive thresholding algorithm. To eliminate the non-TB bacilli from coarse level segmentation, shape descriptors like area, perimeter, convex hull, major axis length and eccentricity are used to extract only the TB bacilli features. Finally, the TB bacilli are counted using the generated bounding boxes to report the level of severity.
Unsupervised anomaly detection for a Smart Autonomous Robotic Assistant Surgeon (SARAS)using a deep residual autoencoder
Apr 22, 2021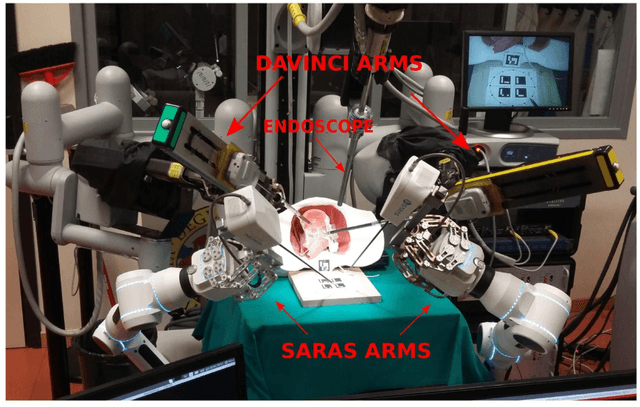
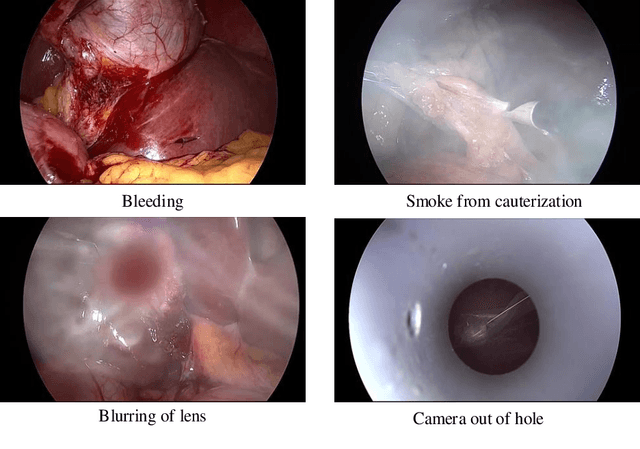
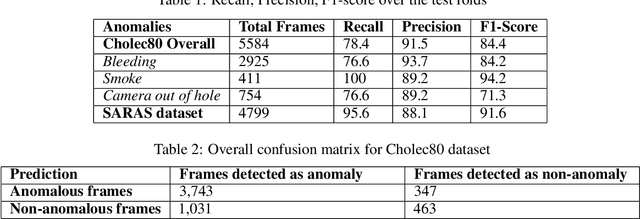
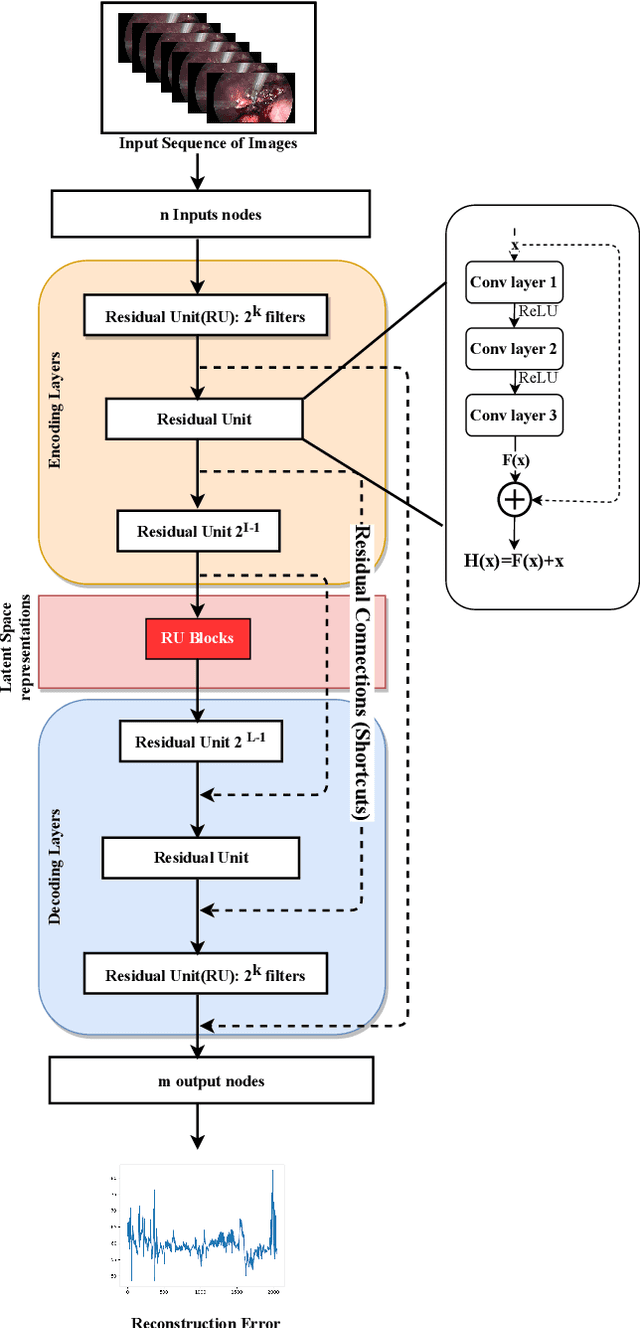
Anomaly detection in Minimally-Invasive Surgery (MIS) traditionally requires a human expert monitoring the procedure from a console. Data scarcity, on the other hand, hinders what would be a desirable migration towards autonomous robotic-assisted surgical systems. Automated anomaly detection systems in this area typically rely on classical supervised learning. Anomalous events in a surgical setting, however, are rare, making it difficult to capture data to train a detection model in a supervised fashion. In this work we thus propose an unsupervised approach to anomaly detection for robotic-assisted surgery based on deep residual autoencoders. The idea is to make the autoencoder learn the 'normal' distribution of the data and detect abnormal events deviating from this distribution by measuring the reconstruction error. The model is trained and validated upon both the publicly available Cholec80 dataset, provided with extra annotation, and on a set of videos captured on procedures using artificial anatomies ('phantoms') produced as part of the Smart Autonomous Robotic Assistant Surgeon (SARAS) project. The system achieves recall and precision equal to 78.4%, 91.5%, respectively, on Cholec80 and of 95.6%, 88.1% on the SARAS phantom dataset. The end-to-end system was developed and deployed as part of the SARAS demonstration platform for real-time anomaly detection with a processing time of about 25 ms per frame.