 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeCross-Learning Between ECG and PCG: Exploring Common and Exclusive Characteristics of Bimodal Electromechanical Cardiac Waveforms
Jun 11, 2025Simultaneous electrocardiography (ECG) and phonocardiogram (PCG) provide a comprehensive, multimodal perspective on cardiac function by capturing the heart's electrical and mechanical activities, respectively. However, the distinct and overlapping information content of these signals, as well as their potential for mutual reconstruction and biomarker extraction, remains incompletely understood, especially under varying physiological conditions and across individuals. In this study, we systematically investigate the common and exclusive characteristics of ECG and PCG using the EPHNOGRAM dataset of simultaneous ECG-PCG recordings during rest and exercise. We employ a suite of linear and nonlinear machine learning models, including non-causal LSTM networks, to reconstruct each modality from the other and analyze the influence of causality, physiological state, and cross-subject variability. Our results demonstrate that nonlinear models, particularly non-causal LSTM, provide superior reconstruction performance, with reconstructing ECG from PCG proving more tractable than the reverse. Exercise and cross-subject scenarios present significant challenges, but envelope-based modeling that utilizes instantaneous amplitude features substantially improves cross-subject generalizability for cross-modal learning. Furthermore, we demonstrate that clinically relevant ECG biomarkers, such as fiducial points and QT intervals, can be estimated from PCG in cross-subject settings. These findings advance our understanding of the relationship between electromechanical cardiac modalities, in terms of both waveform characteristics and the timing of cardiac events, with potential applications in novel multimodal cardiac monitoring technologies.
Electromechanical Dynamics of the Heart: A Study of Cardiac Hysteresis During Physical Stress Test
Oct 25, 2024



Cardiovascular diseases are best diagnosed using multiple modalities that assess both the heart's electrical and mechanical functions. While effective, imaging techniques like echocardiography and nuclear imaging are costly and not widely accessible. More affordable technologies, such as simultaneous electrocardiography (ECG) and phonocardiography (PCG), may provide valuable insights into electromechanical coupling and could be useful for prescreening in low-resource settings. Using physical stress test data from the EPHNOGRAM ECG-PCG dataset, collected from 23 healthy male subjects (age: 25.4+/-1.9 yrs), we investigated electromechanical intervals (RR, QT, systolic, and diastolic) and their interactions during exercise, along with hysteresis between cardiac electrical activity and mechanical responses. Time delay analysis revealed distinct temporal relationships between QT, systolic, and diastolic intervals, with RR as the primary driver. The diastolic interval showed near-synchrony with RR, while QT responded to RR interval changes with an average delay of 10.5s, and the systolic interval responded more slowly, with an average delay of 28.3s. We examined QT-RR, systolic-RR, and diastolic-RR hysteresis, finding narrower loops for diastolic RR and wider loops for systolic RR. Significant correlations (average:0.75) were found between heart rate changes and hysteresis loop areas, suggesting the equivalent circular area diameter as a promising biomarker for cardiac function under exercise stress. Deep learning models, including Long Short-Term Memory and Convolutional Neural Networks, estimated the QT, systolic, and diastolic intervals from RR data, confirming the nonlinear relationship between RR and other intervals. Findings highlight a significant cardiac memory effect, linking ECG and PCG morphology and timing to heart rate history.
Mythological Medical Machine Learning: Boosting the Performance of a Deep Learning Medical Data Classifier Using Realistic Physiological Models
Dec 28, 2021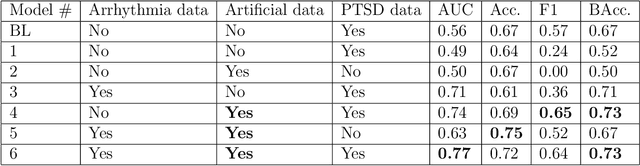
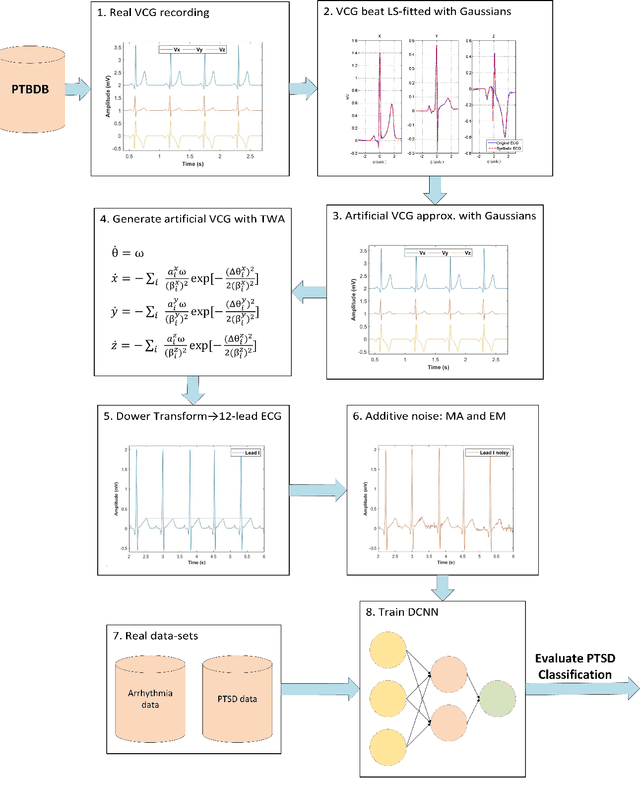
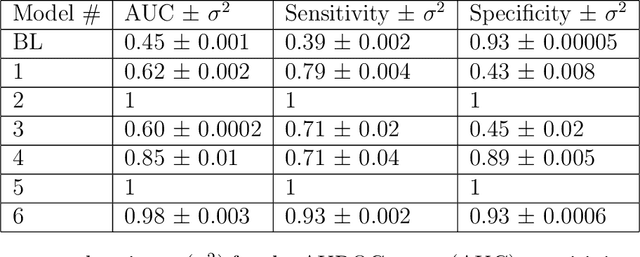
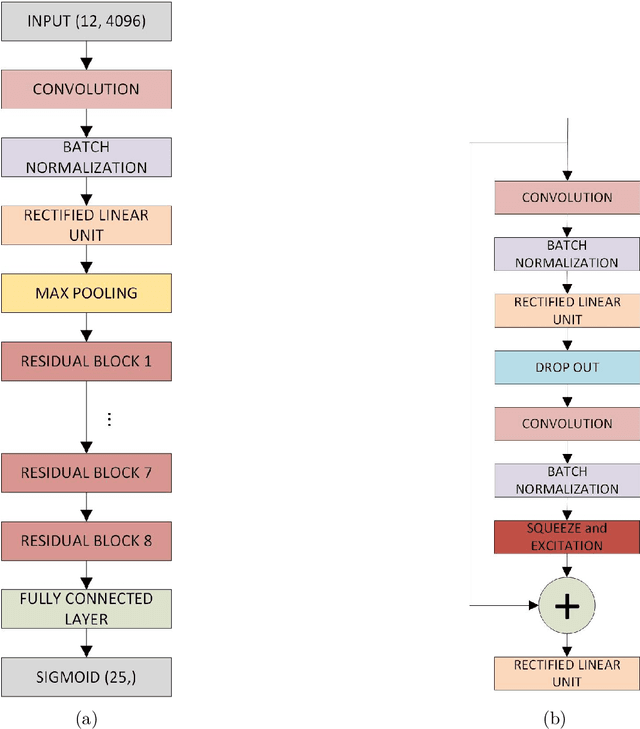
Objective: To determine if a realistic, but computationally efficient model of the electrocardiogram can be used to pre-train a deep neural network (DNN) with a wide range of morphologies and abnormalities specific to a given condition - T-wave Alternans (TWA) as a result of Post-Traumatic Stress Disorder, or PTSD - and significantly boost performance on a small database of rare individuals. Approach: Using a previously validated artificial ECG model, we generated 180,000 artificial ECGs with or without significant TWA, with varying heart rate, breathing rate, TWA amplitude, and ECG morphology. A DNN, trained on over 70,000 patients to classify 25 different rhythms, was modified the output layer to a binary class (TWA or no-TWA, or equivalently, PTSD or no-PTSD), and transfer learning was performed on the artificial ECG. In a final transfer learning step, the DNN was trained and cross-validated on ECG from 12 PTSD and 24 controls for all combinations of using the three databases. Main results: The best performing approach (AUROC = 0.77, Accuracy = 0.72, F1-score = 0.64) was found by performing both transfer learning steps, using the pre-trained arrhythmia DNN, the artificial data and the real PTSD-related ECG data. Removing the artificial data from training led to the largest drop in performance. Removing the arrhythmia data from training provided a modest, but significant, drop in performance. The final model showed no significant drop in performance on the artificial data, indicating no overfitting. Significance: In healthcare, it is common to only have a small collection of high-quality data and labels, or a larger database with much lower quality (and less relevant) labels. The paradigm presented here, involving model-based performance boosting, provides a solution through transfer learning on a large realistic artificial database, and a partially relevant real database.
Late fusion of machine learning models using passively captured interpersonal social interactions and motion from smartphones predicts decompensation in heart failure
Apr 04, 2021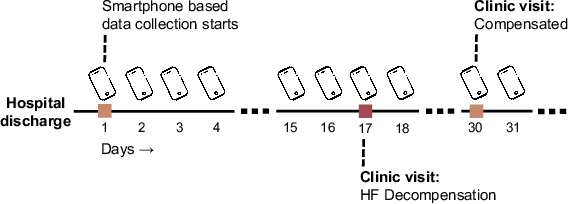
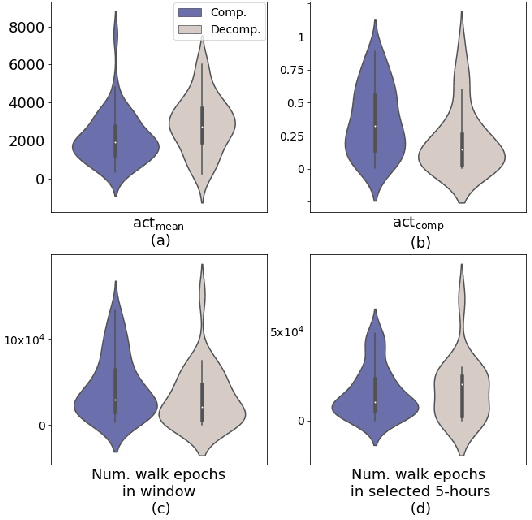
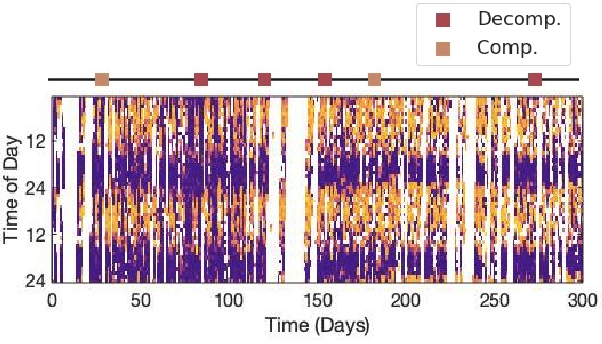
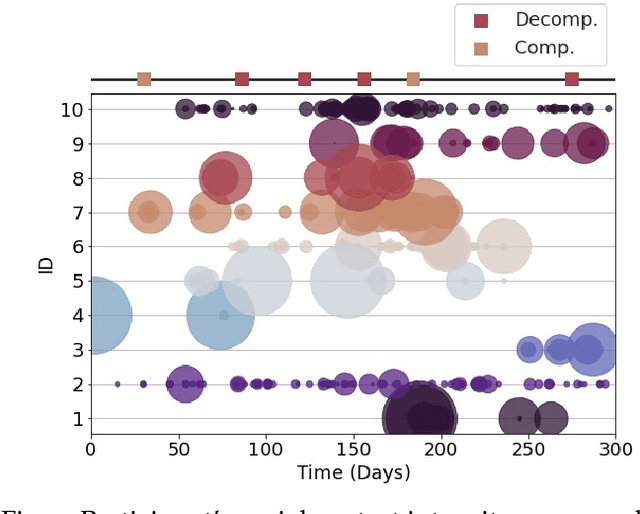
Objective: Worldwide, heart failure (HF) is a major cause of morbidity and mortality and one of the leading causes of hospitalization. Early detection of HF symptoms and pro-active management may reduce adverse events. Approach: Twenty-eight participants were monitored using a smartphone app after discharge from hospitals, and each clinical event during the enrollment (N=110 clinical events) was recorded. Motion, social, location, and clinical survey data collected via the smartphone-based monitoring system were used to develop and validate an algorithm for predicting or classifying HF decompensation events (hospitalizations or clinic visit) versus clinic monitoring visits in which they were determined to be compensated or stable. Models based on single modality as well as early and late fusion approaches combining patient-reported outcomes and passive smartphone data were evaluated. Results: The highest AUCPr for classifying decompensation with a late fusion approach was 0.80 using leave one subject out cross-validation. Significance: Passively collected data from smartphones, especially when combined with weekly patient-reported outcomes, may reflect behavioral and physiological changes due to HF and thus could enable prediction of HF decompensation.
Detection of Paroxysmal Atrial Fibrillation using Attention-based Bidirectional Recurrent Neural Networks
May 07, 2018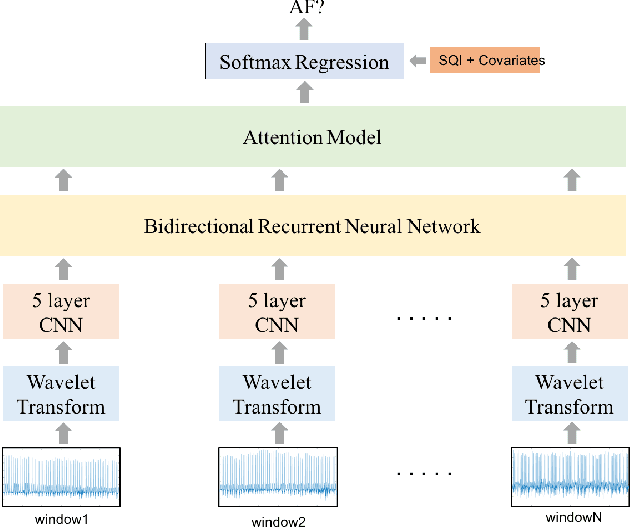
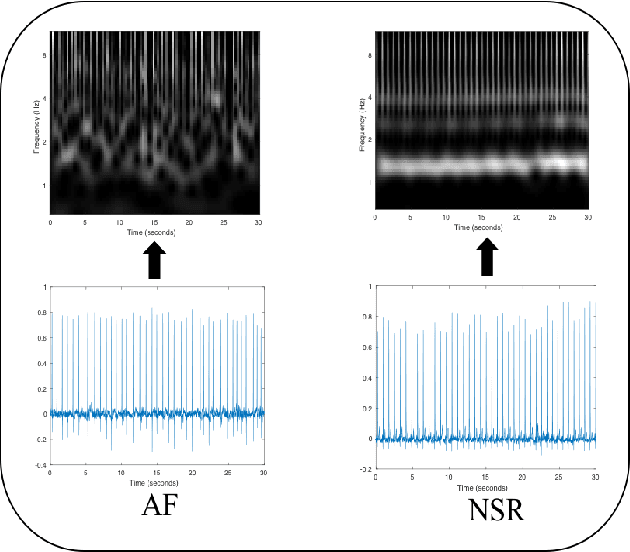
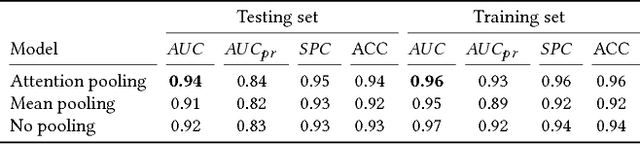
Detection of atrial fibrillation (AF), a type of cardiac arrhythmia, is difficult since many cases of AF are usually clinically silent and undiagnosed. In particular paroxysmal AF is a form of AF that occurs occasionally, and has a higher probability of being undetected. In this work, we present an attention based deep learning framework for detection of paroxysmal AF episodes from a sequence of windows. Time-frequency representation of 30 seconds recording windows, over a 10 minute data segment, are fed sequentially into a deep convolutional neural network for image-based feature extraction, which are then presented to a bidirectional recurrent neural network with an attention layer for AF detection. To demonstrate the effectiveness of the proposed framework for transient AF detection, we use a database of 24 hour Holter Electrocardiogram (ECG) recordings acquired from 2850 patients at the University of Virginia heart station. The algorithm achieves an AUC of 0.94 on the testing set, which exceeds the performance of baseline models. We also demonstrate the cross-domain generalizablity of the approach by adapting the learned model parameters from one recording modality (ECG) to another (photoplethysmogram) with improved AF detection performance. The proposed high accuracy, low false alarm algorithm for detecting paroxysmal AF has potential applications in long-term monitoring using wearable sensors.