 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeAmbulatory blood pressure monitoring versus office blood pressure measurement: Are there sex differences?
Jun 04, 2021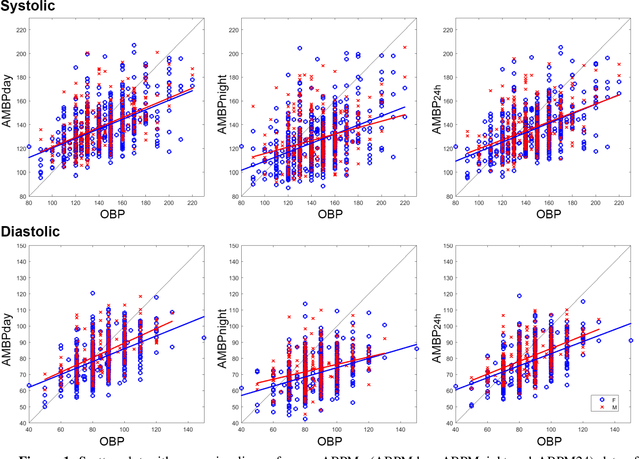
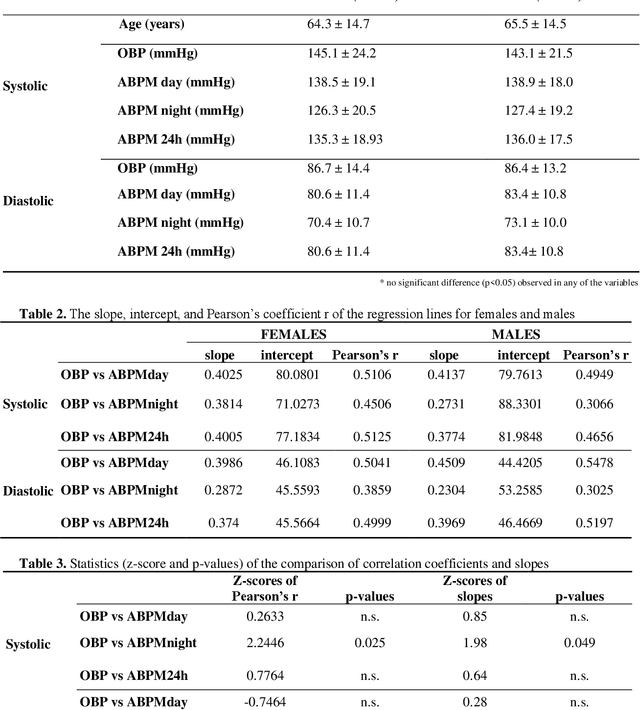
The accurate measurement of blood pressure (BP) is an important prerequisite for the reliable diagnosis and efficient management of hypertension and other medical conditions. Office Blood Pressure Measurement (OBP) is a technique performed in-office with the sphygmomanometer, while Ambulatory Blood Pressure Monitoring (ABPM) is a technique that measures blood pressure during 24h. The BP fluctuations also depend on other factors such as physical activity, temperature, mood, age, sex, any pathologies, a hormonal activity that may intrinsically influence the differences between OBP and ABPM. The aim of this study is to examine the possible influence of sex on the discrepancies between OBP and ABPM in 872 subjects with known or suspected hypertension. A significant correlation was observed between OBP and ABPM mean values calculated during the day, night and 24h (ABPMday, ABPMnight, ABPM24h) in both groups (p<0.0001). The main finding of this study is that no difference between sexes was observed in the relation between OBP and mean ABMP values except between systolic OBP and systolic ABPM during the night. In addition, this study showed a moderate correlation between BPs obtained with the two approaches with a great dispersion around the regression line which suggests that the two approaches cannot be used interchangeably.
EEG changes and motor deficits in Parkinson's disease patients: Correlation of motor scales and EEG power bands
Jun 04, 2021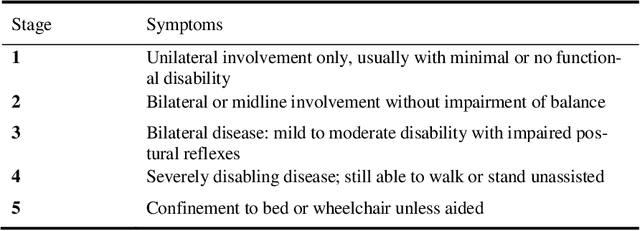
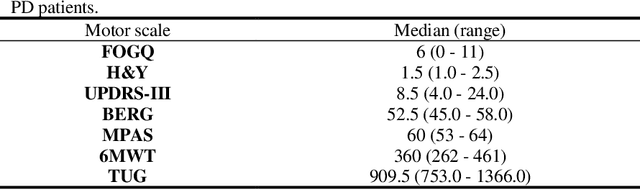
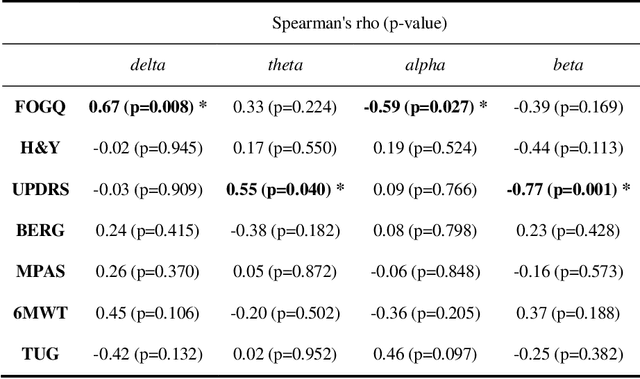
Over the years motor deficit in Parkinson's Disease (PD) patients was largely studied, however, no consistent pattern of relations between quantitative electroencephalography (qEEG) and motor scales emerged. There is a general lack of information on the relation between EEG changes and scales related to specific motor deficits. Therefore, the study aimed to investigate the relation between brain oscillatory activity alterations (EEG power bands) and most used PD-related motor deficit scales. A positive correlation was found between the freezing of the gait questionnaire (FOGQ) and delta spectral power band (rho=0.67; p=0.008), while a negative correlation with the same scale was observed in the alpha spectral power band (rho=-0.59, p=0.027). Additionally, motor scores measure by motor part of Unified Parkinson's Disease Rating Scale (UPDRS) correlated directly with theta (rho=0.55, p=0.040) and inversely with beta EEG power band (rho=-0.77, p=0.001). No significant correlation was found between spectral powers and Hoehn and Yahr (H&Y), BERG (Berg K. et. al. 1995), Modified Parkinson Activity Scale (MPAS), Six-Minute Walk Test (6MWT) and Timed Up and Go Test (TUG). In conclusion, our study supports the earlier findings suggesting a link between EEG slowing and motor decline, providing more insight into the relation between EEG alteration and deficits in different motor domains. These findings indicate that EEG assessment may be a useful biomarker for objective monitoring of progression and neurophysiological effect of rehabilitation approaches in PD's.
Novel Classification of Ischemic Heart Disease Using Artificial Neural Network
Nov 19, 2020Ischemic heart disease (IHD), particularly in its chronic stable form, is a subtle pathology due to its silent behavior before developing in unstable angina, myocardial infarction or sudden cardiac death. Machine learning techniques applied to parameters extracted form heart rate variability (HRV) signal seem to be a valuable support in the early diagnosis of some cardiac diseases. However, so far, IHD patients were identified using Artificial Neural Networks (ANNs) applied to a limited number of HRV parameters and only to very few subjects. In this study, we used several linear and non-linear HRV parameters applied to ANNs, in order to confirm these results on a large cohort of 965 sample of subjects and to identify which features could discriminate IHD patients with high accuracy. By using principal component analysis and stepwise regression, we reduced the original 17 parameters to five, used as inputs, for a series of ANNs. The highest accuracy of 82% was achieved using meanRR, LFn, SD1, gender and age parameters and two hidden neurons.
Transfer Learning improves MI BCI models classification accuracy in Parkinson's disease patients
Oct 29, 2020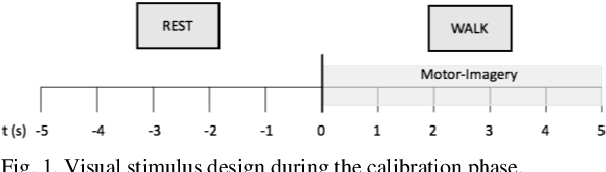
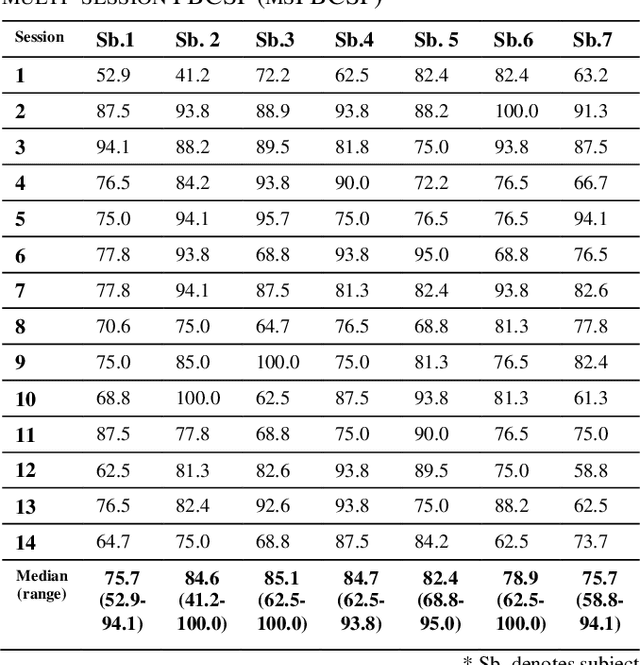
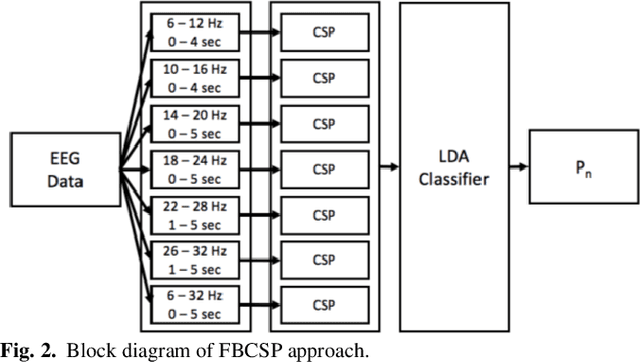
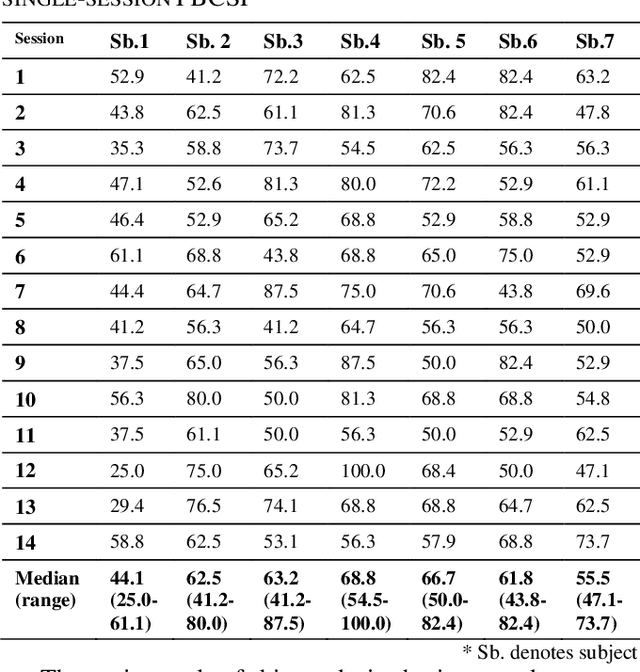
Motor-Imagery based BCI (MI-BCI) neurorehabilitation can improve locomotor ability and reduce the deficit symptoms in Parkinson's Disease patients. Advanced Motor-Imagery BCI methods are needed to overcome the accuracy and time-related MI BCI calibration challenges in such patients. In this study, we proposed a Multi-session FBCSP (msFBCSP) based on inter-session transfer learning and we investigated its performance compared to the single-session based FBSCP. The main result of this study is the significantly improved accuracy obtained by proposed msFBCSP compared to single-session FBCSP in PD patients (median 81.3%, range 41.2-100.0% vs median 61.1%, range 25.0-100.0%, respectively; p<0.001). In conclusion, this study proposes a transfer learning-based multi-session based FBCSP approach which allowed to significantly improve calibration accuracy in MI BCI performed on PD patients.
Identification of Ischemic Heart Disease by using machine learning technique based on parameters measuring Heart Rate Variability
Oct 29, 2020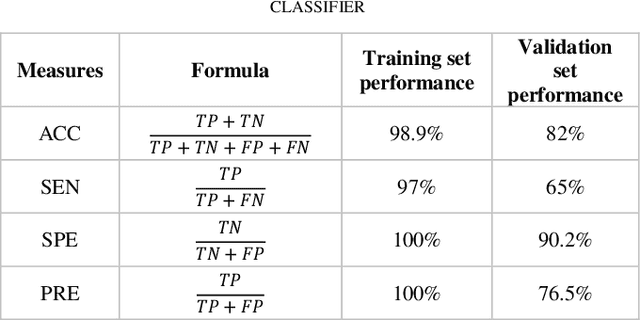
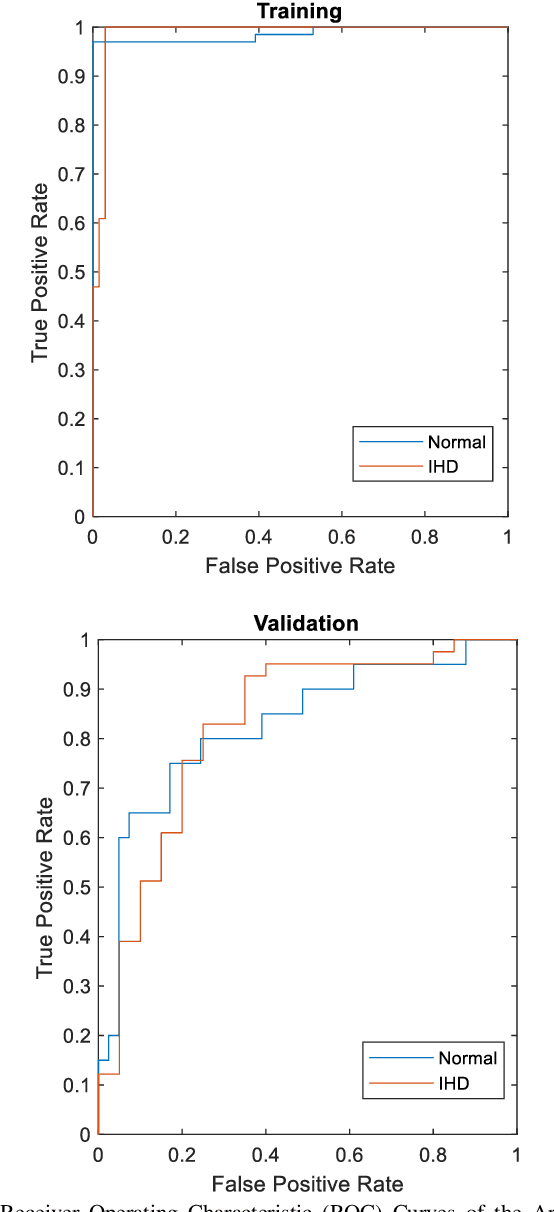
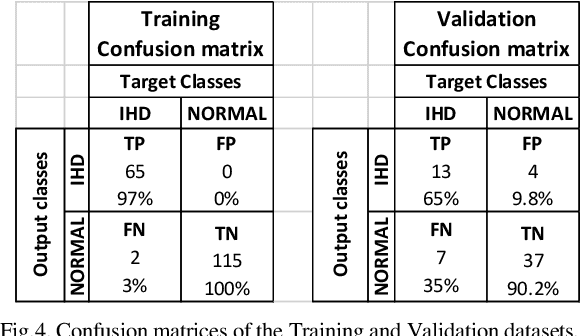
The diagnosis of heart diseases is a difficult task generally addressed by an appropriate examination of patients clinical data. Recently, the use of heart rate variability (HRV) analysis as well as of some machine learning algorithms, has proved to be a valuable support in the diagnosis process. However, till now, ischemic heart disease (IHD) has been diagnosed on the basis of Artificial Neural Networks (ANN) applied only to signs, symptoms and sequential ECG and coronary angiography, an invasive tool, while could be probably identified in a non-invasive way by using parameters extracted from HRV, a signal easily obtained from the ECG. In this study, 18 non-invasive features (age, gender, left ventricular ejection fraction and 15 obtained from HRV) of 243 subjects (156 normal subjects and 87 IHD patients) were used to train and validate a series of several ANN, different for number of input and hidden nodes. The best result was obtained using 7 input parameters and 7 hidden nodes with an accuracy of 98.9% and 82% for the training and validation dataset, respectively.
Performance of Dual-Augmented Lagrangian Method and Common Spatial Patterns applied in classification of Motor-Imagery BCI
Oct 13, 2020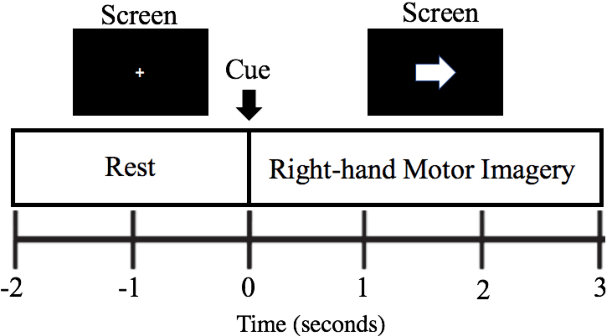
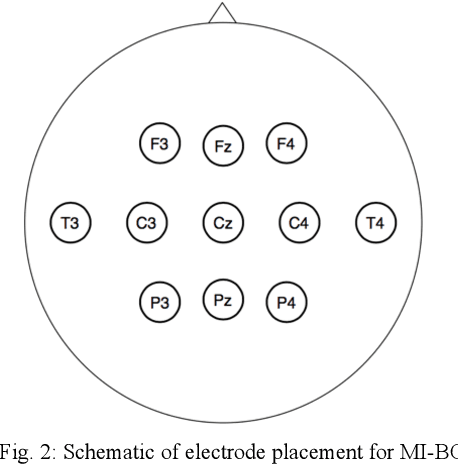
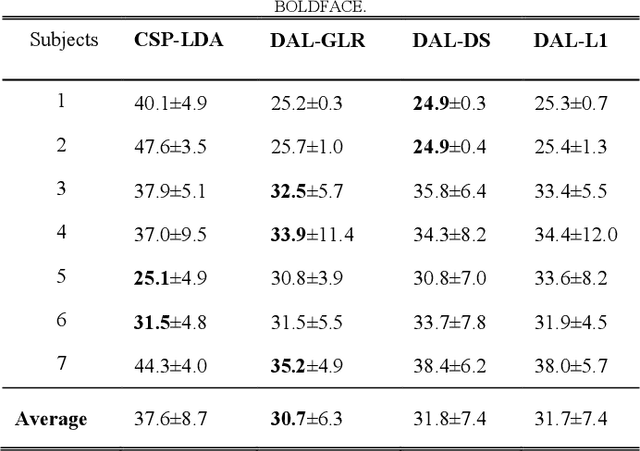
Motor-imagery based brain-computer interfaces (MI-BCI) have the potential to become ground-breaking technologies for neurorehabilitation, the reestablishment of non-muscular communication and commands for patients suffering from neuronal disorders and disabilities, but also outside of clinical practice, for video game control and other entertainment purposes. However, due to the noisy nature of the used EEG signal, reliable BCI systems require specialized procedures for features optimization and extraction. This paper compares the two approaches, the Common Spatial Patterns with Linear Discriminant Analysis classifier (CSP-LDA), widely used in BCI for extracting features in Motor Imagery (MI) tasks, and the Dual-Augmented Lagrangian (DAL) framework with three different regularization methods: group sparsity with row groups (DAL-GLR), dual-spectrum (DAL-DS) and l1-norm regularization (DAL-L1). The test has been performed on 7 healthy subjects performing 5 BCI-MI sessions each. The preliminary results show that DAL-GLR method outperforms standard CSP-LDA, presenting 6.9% lower misclassification error (p-value = 0.008) and demonstrate the advantage of DAL framework for MI-BCI.